Download

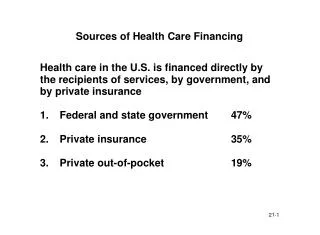
1 / 22
270 likes | 478 Views
18th International Congress on Women’s Health “CITIES AND WOMEN’S HEALTH: GLOBAL PERSPECTIVES ” University of Pennsylvania, Philadelphia, USA, April 7- 10, 2010. Humanization of Childbirth: A Worthwhile Investment for Health Care Services, Professionals, Clients and Communities

E N D
18th International Congress on Women’s Health“CITIES AND WOMEN’S HEALTH: GLOBAL PERSPECTIVES” University of Pennsylvania, Philadelphia, USA, April 7- 10, 2010 Humanization of Childbirth: A Worthwhile Investment for Health Care Services, Professionals, Clients and Communities Veronica Reis, MD, MPH – MCHIP Mozambique Lidia Chongo, MD – MoH Mozambique
OBJECTIVE OF THE SESSION • To share the results of efforts undertaken in Mozambique to promote the quality and humanization of healthcare, particularly in the area of childbirth.
Humanization of ChildbirthDEFINITION • “Humanization of childbirth” is an approach that centers on the individual, emphasizes the fundamental rights of the mother, newborn and families, and promotes birthing practices that recognize women’s preferences and needs.
Considerations: evolution of the medical practices favors the “technocratic model” • The body as a machine • Separation between the body and the mind
Symbols of the “technocratic Model” • Centered on the professional • Unpowerment of the woman
Symbols of the “Technocratic Model” Use of no evidence based Practices
Symbols of the “Technocratic Model” Woman solitary
Humanization of Childbirth includes: • Respecting beliefs traditions and culture; • The right to information and privacy, • Choice of a companion during childbirth; • Liberty of movement during the labor
Humanization of Childbirth includes: • Choice of position for childbirth; • Skin-to-skin contact of the newborn; • Use of evidence based practices; • Guarantee of Emergence Obstetric and Neonatal Care, if necessary;
Humanization of Childbirth in Mozambique
MOZAMBIQUE CONTEXT • Population: 20 million • Among the 10 poorest countries in the world • Life expectancy at birth: 45 years • HIV prevalence: 16.2% • Maternal mortality: 408/100,000 live births • Neonatal mortality: 48/ 1000 live births Source: 2007census, DHS 2003 Photo: Ismael Miquidade
Main problems on the Health System detected by the Moz MoH • Shortfall infrastructure, lack of material and limited human resource in quantity and quality • Poor management of health services • Long waiting times • Lack of a welcoming reception • lack of privacy and limited information provided to the client • Lack of satisfaction by the clients and health workers. Source: MoH Moz, 2007.
Investing in quality improvement and humanization of health care • In 2006, the Mozambique Ministry of Health (MOH), with support from international partners, developed a National Plan to Improve the Quality and Humanization of Maternal and Child Health (MCH) Services that adopted a quality improvement methodology developed by Jhpiego: Standards-Based Management and Recognition (SBM-R)
Standards-Based Management and Recognition (SBM-R) • It is a practical approach that follows four main steps: • Setting performance standards based on national norms and international references; • Implementing standards through a systematic methodology; • Measuring progress to guide improvement toward standards; • Recognizing achievement of the standards.
2007-2008: Quality improvement process in 6 Provinces / 18 HC • Results by the end of 2008: Facilities doubled or tripled their performance after one year. Operating at a higher quality level, adhering to established evidence-based standards. • As a result, the MOH expanded the quality and humanization improvement process in 2009 to the 34 biggest hospitals in all country. This program now is called the Model Maternity Initiative.
Rural Hospital of ManjacazeAn example of this movement! • At Manjacaze Hospital, located in the south of Mozambique in Gaza Province, staff has been working with the local community to guide the transformation of the hospital into a welcoming environment for clients, and humanization principles have been successfully incorporated into services. • These efforts have resulted in increased health worker and client satisfaction and demand for services.
At Manjacaze Hospital Humanization efforts included • Trainning staff on the implementation of the MNH standards • Dissemination of information about humanization and quality of care, and client rights; • Ensure the implementation of humanized childbirth and MNH high impact interventions practices: • allowing women to be accompanied during labor and childbirth. • Liberty of movement during labor • allowing women to choose a position during childbirth • Skin-to-skin contact of the newborn; • Active managment of the third labor to prevent PPH .
Client satisfaction • One mother allowed to accompany her daughter during childbirth said: “This is what I can call a trully independence!”. • One young Mozambican woman that gave birth to her first child under humanized conditions, in a squatting position and accompanied by her partner is now sharing her experiences with other women and communities in Mozambique, affirming, “We women must speak up to fight for our rights”. And the father of the baby said: “It was the most incredible experience of my life”.
Conclusion • Humanizing healthcare can improve quality of care, increase service utilization and client satisfaction. • While more research is needed to measure the benefits of humanizing healthcare, current analysis of experiences in Mozambique demonstrate humanizing healthcare is a worthwhile investment.
References • ACCESS. Module 4: Women-friendly Care. In: Best Practices in Maternal and Newborn Care: Learning Resource Package. Jhpiego-Johns Hopkins University. Baltimore-MD, USA. 2008. • Davis-Floyd R., St.Jonh G. From Doctor to Healer: The transformative Journey. New Brunswick NJ: Rutgers University Press. 1998. • Gupta and Nikodem. Maternal posture in labour. Eur J ObstetGynecolReprodBiol 2000 Oct;92(2): 273-277. • Jones R. O Homem de Vidro: Memórias de um obstetra humanista. Porto Alegre-BR: Idéias a Granel, 2004. • Maadi et al. Effects of female relative support in labor: A randomized controlled trial. Birth. 1999 Mar; 26(1): 4-8. Erratum in: Birth 1999 Jun; 26(2): 137. • MISAU. Atenção humanizada a mulher e ao recém-nascido durante o parto e o nascimento. Ministério da Saúde. Moçambique, 2007a. • MISAU. Plano Estratégico do Sector Saúde 2007-2012. Ministério da Saúde. Moz, 2007b.