Download
1 / 1
10 likes | 195 Views
Methods Data was collected retrospectively on all patients receiving a renal transplant from January 2007 to December 2011. The operation note and clinical records for each patient were reviewed. Any ureteric complications and the subsequent management were noted. Introduction

E N D
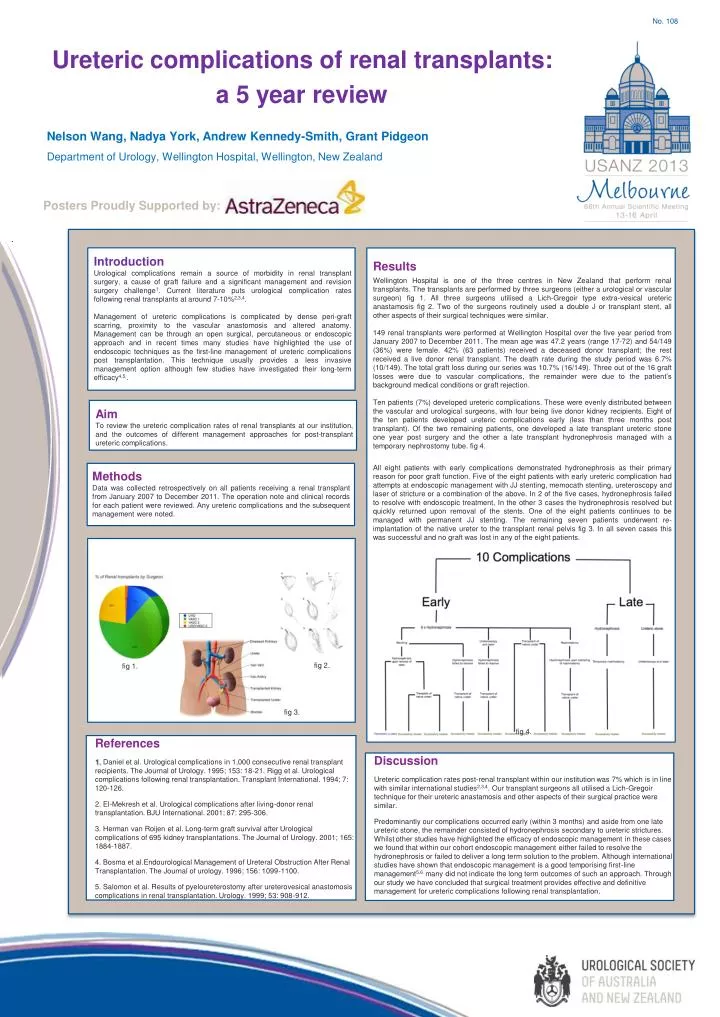
Methods Data was collected retrospectively on all patients receiving a renal transplant from January 2007 to December 2011. The operation note and clinical records for each patient were reviewed. Any ureteric complications and the subsequent management were noted. Introduction Urological complications remain a source of morbidity in renal transplant surgery, a cause of graft failure and a significant management and revision surgery challenge1. Current literature puts urological complication rates following renal transplants at around 7-10%2,3,4. Management of ureteric complications is complicated by dense peri-graft scarring, proximity to the vascular anastomosis and altered anatomy. Management can be through an open surgical, percutaneous or endoscopic approach and in recent times many studies have highlighted the use of endoscopic techniques as the first-line management of ureteric complications post transplantation. This technique usually provides a less invasive management option although few studies have investigated their long-term efficacy4,5,. Results Wellington Hospital is one of the three centres in New Zealand that perform renal transplants. The transplants are performed by three surgeons (either a urological or vascular surgeon) fig 1. All three surgeons utilised a Lich-Gregoir type extra-vesical ureteric anastamosis fig 2. Two of the surgeons routinely used a double J or transplant stent, all other aspects of their surgical techniques were similar. 149 renal transplants were performed at Wellington Hospital over the five year period from January 2007 to December 2011. The mean age was 47.2 years (range 17-72) and 54/149 (36%) were female. 42% (63 patients) received a deceased donor transplant; the rest received a live donor renal transplant. The death rate during the study period was 6.7% (10/149). The total graft loss during our series was 10.7% (16/149). Three out of the 16 graft losses were due to vascular complications, the remainder were due to the patient’s background medical conditions or graft rejection. Ten patients (7%) developed ureteric complications. These were evenly distributed between the vascular and urological surgeons, with four being live donor kidney recipients. Eight of the ten patients developed ureteric complications early (less than three months post transplant). Of the two remaining patients, one developed a late transplant ureteric stone one year post surgery and the other a late transplant hydronephrosis managed with a temporary nephrostomy tube. fig 4. All eight patients with early complications demonstrated hydronephrosis as their primary reason for poor graft function. Five of the eight patients with early ureteric complication had attempts at endoscopic management with JJ stenting, memocath stenting, ureteroscopy and laser of stricture or a combination of the above. In 2 of the five cases, hydronephrosis failed to resolve with endoscopic treatment, In the other 3 cases the hydronephrosis resolved but quickly returned upon removal of the stents. One of the eight patients continues to be managed with permanent JJ stenting. The remaining seven patients underwent re-implantation of the native ureter to the transplant renal pelvis fig 3. In all seven cases this was successful and no graft was lost in any of the eight patients. Aim To review the ureteric complication rates of renal transplants at our institution, and the outcomes of different management approaches for post-transplant ureteric complications. No. 108 Ureteric complications of renal transplants: a 5 year review Nelson Wang, Nadya York, Andrew Kennedy-Smith, Grant Pidgeon Department of Urology, Wellington Hospital, Wellington, New Zealand Posters Proudly Supported by: fig 2. fig 1. fig 3. fig 4. • References • Daniel et al. Urological complications in 1,000 consecutive renal transplant recipients. The Journal of Urology. 1995; 153: 18-21. Rigg et al. Urological complications following renal transplantation. Transplant International. 1994; 7: 120-126. • El-Mekresh et al. Urological complications after living-donor renal transplantation. BJU International. 2001; 87: 295-306. • Herman van Roijen et al. Long-term graft survival after Urological complications of 695 kidney transplantations. The Journal of Urology. 2001; 165: 1884-1887. • Bosma et al.Endourological Management of Ureteral Obstruction After Renal Transplantation. The Journal of urology. 1996; 156: 1099-1100. • Salomon et al. Results of pyeloureterostomy after ureterovesical anastomosis complications in renal transplantation. Urology. 1999; 53: 908-912. Discussion Ureteric complication rates post-renal transplant within our institution was 7% which is in line with similar international studies2,3,4. Our transplant surgeons all utilised a Lich-Gregoir technique for their ureteric anastamosis and other aspects of their surgical practice were similar. Predominantly our complications occurred early (within 3 months) and aside from one late ureteric stone, the remainder consisted of hydronephrosis secondary to ureteric strictures. Whilst other studies have highlighted the efficacy of endoscopic management in these cases we found that within our cohort endoscopic management either failed to resolve the hydronephrosis or failed to deliver a long term solution to the problem. Although international studies have shown that endoscopic management is a good temporising first-line management5,6 many did not indicate the long term outcomes of such an approach. Through our study we have concluded that surgical treatment provides effective and definitive management for ureteric complications following renal transplantation.