Download
1 / 21
210 likes | 348 Views
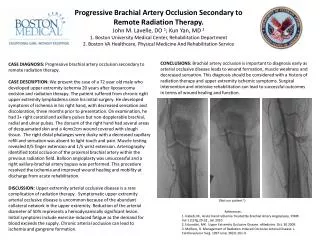
CFD final Project Modeling the Access Point on the Brachial Artery. Novemer 16, 2010 Nicole Varble. Problem Definition- Overview. Problem- Patients on hemodialysis need an access point Native vessels become overstressed

E N D
CFD final Project Modeling the Access Point on the Brachial Artery Novemer 16, 2010 Nicole Varble
Problem Definition- Overview • Problem- Patients on hemodialysis need an access point • Native vessels become overstressed • Solution- Create an access vessel between an artery and vein in the arm • High flow • Low Pressure • Can be punctured repeatedly • Resulting Problem- Adequate flow does not reach the hand • Blood flow is redirected through access vessel • Hand is deprived of nutrients Hand Artery Vein Figure 1: Native Circulation Area of Interest Hand Artery AVF Vein Figure 2: Native Circulation w/ AVF
Problem Definition- Overview 1. Proximal Brachial Artery 2. Distal Brachial Artery Hand Proximal Distal Brachial Artery AVF Vein Figure 3 4. Antegrade Flow- Forward 5. Retrograde Flow- Backwards Hand Hand Figure 5 Figure 4
Project Definition- Overview • Goal: Gain insight to the flow patterns at the intersection of native artery and access vessel • Interests comes from my thesis work • Model of the entire arm’s vasculature • Native circulation (NC), NC with access, NC with access and DRIL (a corrective procedure) • For this project only interested in what happens at the intersection point • Little research on the topic Brachial Artery Area of Interest Access Vessel Figure 6: Brachialcephalicateriovenous fistula D.J. Minion, E. Moore, E. Endean, and K. (Lexington, "Revision Using Distal Inflow: A Novel Approach to Dialysis- associated Steal Syndrome," Annals of Vascular Surgery, vol. 19, 2005, pp. 625- 628.
Project Definition- Aims • Aim 1: Create the geometry based on the average blood vessel diameter, length and boundary conditions. Analyze the entrance to the access vessel and the magnitude and direction of flow to the hand. • Aim 2: Change the boundary conditions to that of a hypertensive patient (elevated blood pressure). Determine flow conditions at the access changed. • Aim 3: If backwards flow does not occur in ‘Aim 1,’ determine the boundary conditions at the outlet for which backwards flow occurs. If backwards flow does occur, determine a threshold at which this does occur and quantify in terms of differential pressure between the two outlets.
Project Definition- Assumptions • Assumptions: • Non- puslitileflow • Blood vessels are idealized a perfect cylinders with sections of constant diameter • Diameters are based on the average size of blood vessels complied from current literature • Inlet and outlet pressures and flows are based on average pressures and flows in the vessels and blood • The working fluid, is considered a non-Newtonian fluid with an average density and dynamic viscosity. Figure 7: 2D schematic of brachial artery and access vessel
Project Definition- Boundary Conditions Table 1: Geometry and Boundary Conditions
Project Definition- Geometry and Boundary Conditions • One velocity inlet (constant) • Proximal brachial artery • Two pressure outlets • Distal brachial artery • Access vessel • Pressure Difference • dP = P1- P2 • Velocity inlet fixed • Only P2 changed Figure 8: 3D geometry created in Gambit Figure 9: Specified Boundary Condition, one inlet velocity and two outlet pressures
Mesh • Edge meshed • Successive ratio = 1.016 • Interval count = 10 • Faces meshed • Quad/pave • Interval count = 10 • Volume meshed • Default Tet/hybrid • Interval size = 1 Figures 9 and 10: Close up image on bifurcation and mesh geometry, the originally meshed (yellow) and originally meshed faces (green) labeled
Mesh- Grid Independent Solution • Percentage of Total Inflow in Distal Brachial Artery • Number of Element Mesh 4 Mesh 2 Mesh 3 Ideal Mesh Figure 11: Analysis of grid independent solution. Knee of the curve (ideal mesh) is identified.
Numerical Procedures • Convergence Set to 1e-6, converged in every case Table 2: Numerical Procedures (choices highlighted in orange)
Results • Analyzed • Aim 1 and 2 • Nature of flow in normal and hypertensive cases • Aim 1, 2 and 3 • Point of maximum flow • Pressure throughout control volume to identify the low pressure vessel • Direction and Magnitude of flow in the distal brachial artery • Outcome • Identify what at what pressure difference retrograde (backwards) flow occurs
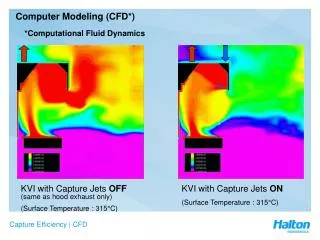
Results- Normal and Hypertensive Case • Possible turbulent regions found at bifurcation • Flow reversal immediately present • When changed to the hypertensive case, only a slight increase in in velocity magnitude, no other change (pressure difference??) Turbulent Region Turbulent Region Flow Reversal Figure 12: Velocity vector plot at normal flow conditions. Note flow reversal in the distal portion of the brachial artery and turbulent regions at the bifurcation
Results- Velocity Magnitude Figures 13 and 14: Velocity Magnitude contour plot. Iso-surface was created along constant z-axis. Maximum velocity occurring just beyond bifurcation in the access vessel and in the proximal brachial artery for dP = to 20 and 5 mmHg respectively
Results- Static Pressure • Contour plot of static pressure on a constant z- surface. • Low pressure vessels are where flow will preferentially travel Figures 15, 16 and 17: Contour plot of static pressure on a constant z- surface. The low pressure vessels where flow will preferentially flow are label.
Results- Direction of Flow Retrograde Flow Retrograde Flow dP = 20 mmHg dP = 8 mmHg Antegrade Flow Antegrade Flow dP = 5 mmHg dP = 0mmHg Figures 18- 21: Velocity vector plots on a constant z- surface. Flow reversal occurs at dP of 20 mmHg and 8 mmHg and forward flow occurs at 5 mmHg and 0 mmHg.
Results- Prediction of Flow Antegrade Retrograde Figure 22: Relationship between differential pressure between distal brachial artery and access vessel and percent of total inflow in distal brachial artery
Results- Summary Table 3: Summary of Results Figure 23: 2D schematic of modeled blood vessel geometry and boundary conditions
Conclusions • Maximum velocity occurs just beyond bifurcation or in proximal brachial artery • All cases, access vessel acts as a low pressure vessel (flow preferentially travels through it) • When differential pressure between outlets is limited to 10 mmHg flow is antegrade • CFD model predicts when retrograde flow in distal brachial artery will occur based on differential pressure • Experimental verification needed • Potentially physicians can use this relationship or something similar to eliminate need for corrective procedures (DRIL)
References • [1] A. Peretz, D.F. Leotta, J.H. Sullivan, C.a. Trenga, F.N. Sands, M.R. Aulet, M. Paun, E.a. Gill, and J.D. Kaufman, "Flow mediated dilation of the brachial artery: an investigation of methods requiring further standardization.," BMC cardiovascular disorders, vol. 7, 2007, p. 11. • [2] J. Zanow, U. Krueger, P. Reddemann, and H. Scholz, "Experimental study of hemodynamics in procedures to treat access-related ischemia," Journal of Vascular Surgery, 2008, pp. 1559-1565. • [3] V. Patnaik, G. Kalsey, and S. Rajan, "Branching Pattern of Brachial Artery-A Morphological Study," J. Anat. Soc. India, vol. 51, 2002, pp. 176-186. • [4] W.S. Gradman, C. Pozrikidis, L. Angeles, and S. Diego, "Analysis of Options for Mitigating Hemodialysis Access-Related Ischemic Steal Phenomena," Annals of Vascular Surgery, vol. 18, 2004, pp. 59-65. • [5] K.A. Illig, S. Surowiec, C.K. Shortell, M.G. Davies, J.M. Rhodes, R.M. Green, and N. York, "Hemodynamics of Distal Revascularization- Interval Ligation," Annals of Vascular Surgery, vol. 19, 2005, pp. 199-207. • [6] C.L. Wixon, J.D. Hughes, and J.L. Mills, "Understanding Strategies for the Treatment of Ischemic Steal Syndrome after Hemodialysis Access," Elsevier Science, 2000, pp. 301-310.