Download
1 / 7
70 likes | 231 Views
Accountable Care Organizations: Healthcare reform provision. Broad range of providers able to initiate ACOs Accountability for total cost, quality and care of beneficiaries 3-year participation commitment Legal structure to receive and distribute savings

E N D
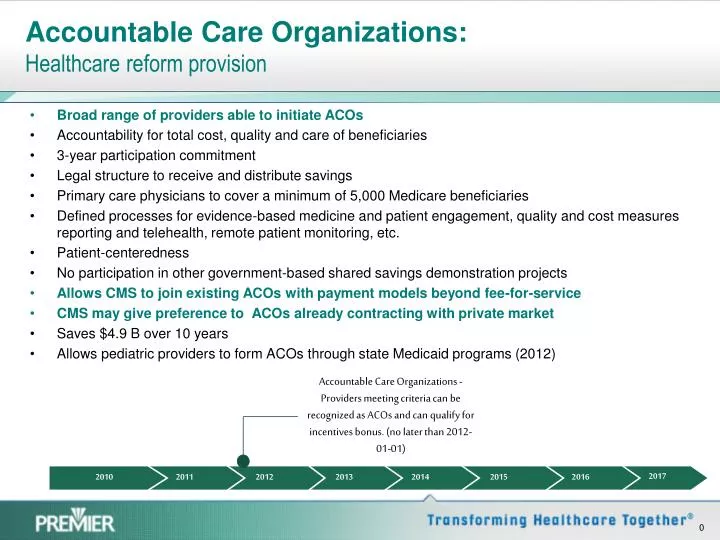
Accountable Care Organizations:Healthcare reform provision Broad range of providers able to initiate ACOs Accountability for total cost, quality and care of beneficiaries 3-year participation commitment Legal structure to receive and distribute savings Primary care physicians to cover a minimum of 5,000 Medicare beneficiaries Defined processes for evidence-based medicine and patient engagement, quality and cost measures reporting and telehealth, remote patient monitoring, etc. Patient-centeredness No participation in other government-based shared savings demonstration projects Allows CMS to join existing ACOs with payment models beyond fee-for-service CMS may give preference to ACOs already contracting with private market Saves $4.9 B over 10 years Allows pediatric providers to form ACOs through state Medicaid programs (2012) Accountable Care Organizations - Providers meeting criteria can be recognized as ACOs and can qualify for incentives bonus. (no later than 2012-01-01) 2017 2010 2011 2012 2013 2014 2015 2016
ACO Participation Requirements:Healthcare Reform Provisions • Providers eligible to participate in ACOs: • Hospitals employing ACO professionals • ACO professionals in group practice arrangements • Networks of individual practices of ACO professionals • Partnerships or joint venture arrangements between hospitals and ACO professionals • Other groups of providers that the Secretary deems appropriate • ACOs must meet certain quality thresholds: • Clinical processes and outcomes • Patient and caregiver perspectives on care • Utilization and costs
Washington Developments • 6/24, 1st CMS listening session • 9/8, Group CMS listening session • 9/13, MedPAC meeting on ACOs • 10/5, FTC/OIG/CMS workshop • 11/13, CMS request for information • Fall/winter 2010, regulation expected
Key design issues • Beneficiary attribution, opt-out, transparency and inducements • Timely access to A, B & D claims data and beneficiary list • Encourage & coordinate with other payers (Medicaid, private) • Legal (anti-trust, anti-kickback…) “safe harbors”/guidance • Models that include broadest group of provider types to maximize impact on communities • Multiple payment models (partial or full capitation) from the start of the program • Shared savings design for small patient populations
Physician Group Practice (PGP) - CMS Demo • Test bed for demonstrating ACO models • Creates incentives for physician groups to coordinate the overall care delivered to Medicare beneficiaries • Shared savings based on improved quality and cost efficiency • Enables collaboration among providers to benefit Medicare beneficiaries • Demo goals (5 year demonstration): • Coordination of Part A and Part B services • Promote cost efficiency and effectiveness through investment in care management programs, process redesign, and tools for physicians and their clinical care teams • Reward physicians for improving health outcomes (32 quality measures) by sharing in financial savings
PGP Participants • PGP participants include 5,000 physicians and 220,000 Medicare fee-for-service beneficiaries: • Billings Clinic, Billings, Montana • Dartmouth-Hitchcock Clinic, Bedford, New Hampshire • The Everett Clinic, Everett, Washington • Forsyth Medical Group, Winston-Salem, North Carolina • Geisinger Health System, Danville, Pennsylvania • Marshfield Clinic, Marshfield, Wisconsin • Middlesex Health System, Middletown, Connecticut • Park Nicollet Health Services, St. Louis Park, Minnesota • St. John’s Health System, Springfield, Missouri • University of Michigan Faculty Group Practice, Ann Arbor, Michigan
PGP Outcomes… So far (as of 8/2009) • Three-year average quality-improvement results: • 10 percentage points on the diabetes, • 11 percentage points on the congestive heart failure measures, • 6 percentage points on the coronary artery disease measures, • 10 percentage points on the cancer screening measures, and • 1 percentage point on the hypertension measures. • Five participants earned $25.3 million in performance payments for improving quality and achieving savings of $32.3 million: • Dartmouth-Hitchcock Clinic • Geisinger Clinic • Marshfield Clinic • St. John’s Health System, and • The University of Michigan Faculty Group Practice