Download
1 / 52
560 likes | 911 Views
FDA Approvals, IND, IDE and Clinical Trials. March 16, 2011 Gerberding Hall 142, University of Washington. Speakers. Lynn Rose, Research Associate Professor, Pediatrics; Director, Regulatory and Clinical Affairs, Seattle Children’s Research Institute

E N D
FDA Approvals, IND, IDE and Clinical Trials March 16, 2011 Gerberding Hall 142, University of Washington
Speakers Lynn Rose, Research Associate Professor, Pediatrics; Director, Regulatory and Clinical Affairs, Seattle Children’s Research Institute Ann Melvin MD, MPH, Associate Professor Pediatrics – Infectious Diseases Seattle Children’s Hospital Co-director Regulatory Support and Bioethics Core - ITHS
Learning Goals of Presentation 3 • Brief history behind FDA regulations and processes • Review IND and IDE Exemptions • Practical Considerations for Writing for INDs and IDEs • Review Investigator Commitments and Common Deficiencies • Overview of resources available through ITHS Confidential
Safety is the Key to Initiating Clinical Trials Long, sad history of both abuses and ignorance leading to clinical disasters: From past disasters come current laws As the years have passed, more and more regulations (i.e. disasters) have been passed People more risk averse 4 Confidential
1937: Sulfanilamide Elixir • S.E. Massengill developed Sulfanilamide Elixir for pediatric indications • Sulfa drug dissolved in diethylene glycol • First death reported in October 1937 • Eventually 107 people died, mostly children • 108th death was the chemist who invented it (suicide) • Dr. Geiling at the U. Chicago showed the solvent was toxic • FDA seizures and prosecution • “Misbranded” – “elixir” implied it contained alcohol, which it didn’t • Massengill Co. paid a fine of $26,100 Confidential
Federal Food, Drug, and Cosmetic Act of 1938 • Increased emphasis on safety: • Manufacturer had to test any new drug for safety and report results to the FDA • No standards for safety testing were established • No requirements for efficacy • Authorized FDA to conduct factory inspections • No manufacturing standards were set • Labeling had to include • All ingredients and quantity of each • Directions for use, Warnings about dangers • Product was considered misbranded if it was dangerous to health when used in the dosage recommended in the label. • No oversight of clinical trials was mandated Confidential
Thalidomide • “Wonder drug” for insomnia, coughs, colds, and headaches. Also an effective antiemetic for morning sickness. • Thalidomide distributed to >1000 U.S. doctors on an “investigational” basis • > 20,000 patients received the drug; 624 were pregnant • Doctors were “invited” to report on their results, but were under no obligation to do so • NDA for thalidomide was assigned to a new FDA examiner, Dr. Frances Kelsey, who had studied in the lab of Dr. Geiling as a graduate student
Dr. Kelsey won the President’s Medal for Distinguished Federal Civilian Service from President John F. Kennedy (highest recognition possible for civil service) Drug reform proposals that had been languishing were resurrected and enacted without a single dissenting vote in either the House or Senate Thalidomide Aftermath Confidential
Kefauver-Harris Amendments of 1962 • FDA gained jurisdiction over testing of drugs before they would be approved for marketing • Drug firms (“sponsors”) had to apply to the FDA to perform human trials of a new drug: Investigational New Drug application, or IND • Sponsors had to inform FDA of what happened during clinical testing • Patients in trials had to give informed consent (WWII aftermath) • Animal testing had to be conducted prior to human testing • Experiments had to be properly planned, and include controls • Investigators conducting trials had to be qualified • Sponsors had to describe the scientific training and experience necessary to test the safety of the drug • Drug had to show efficacy before it could be marketed • Established Good Manufacturing Practices Confidential
Medical Device Amendments of 1976 Following the Dalkon Shield Deaths: • Law passed to ensure safety and effectiveness of medical devices, including diagnostics • Required manufacturers to register with FDA and follow standard quality control procedures • Identified 3 classes of medical devices, each with unique requirements for marketing authorization • Class I – lowest risk devices and lowest set of requirements • Clinical testing not required for marketing approval • No regulatory application (i.e. 510 (k) or PMA required for marketing authorization) • Class II –medium risk devices, higher performance standards required • Marketing authorization requires 510 (k) application • Clinical testing may be required if product has no “predicate” as comparator • Class III – highest risk devices, highest level of performance standards • Investigational Device Exemption (IDE) • Premarket Authorization (PMA) for Marketing Approval Confidential
Medical Device Classes: Class I General Controls Most exempt from premarket submission Class II Special Controls Premarket Notification [510(k)] Class III Premarket Approval Require Premarket Application [PMA] Examples of Medical Device Classifications • Additional Classification: • “De Novo” • Device "types" that have never been marketed in the U.S., but whose safety profile and technology are now reasonably well understood • Humanitarian Device Exemption (HDE) • Devices for orphan diseases • Intended to benefit patients in diagnosis and/or treatment of disease or condition affecting or manifested in fewer than 4,000 patients per year in the United States
Since 1976… 13 • The regulations embodied in the Food and Drug Administration Modernization Act (1997) have continued to evolve as new problems emerge • Requirements for post-market surveillance protocols • Safety data continues to be prioritized by FDA (over efficacy) when reviewing IND applications because history shows that safety risks lurk in unusual places • Cell lines (e.g., viral, mycoplasm contamination) • Expression Systems (e.g. antibiotic selection) • Formulation (e.g., sulfanilamide) • Contaminants from manufacturing • Guidance Documents have proliferated to aid investigators in understanding the requirements for INDs and IDEs • Product and Indication Specific Confidential
Understanding the Regulations for INDs and IDEs • Review 21 CFR Part 312- Investigational New Drug Application • Review 21 CFR Part 812 – Investigational Device Exemptions • Table of Contents Clearly Delineated • Review FDA Guidance Documents related to product type, disease, animal models, etc. • Consider a Pre-IND/IDE meeting: • Before you embark on animal safety studies • Once preclinical data is sufficient to have a meaningful discussion. • To clarify the product classification and FDA review division • To determine if study is eligible for IND or IDE waiver Confidential
Investigational New Drug (IND) Applications • IND applications are required for clinical studies of investigational drugs that are not “exempt” from the IND regulations • Investigational drugs means a “new” drug or biological drug that is used in a clinical investigation. • The term “new” encompasses both unapproved drugs and approved drugs that are used in new ways (i.e., new indications) Confidential
Conditions for IND Exemption • Conditions for IND Waivers are provided in 21 CFR Part 312.2 • Study results will not be reported to FDA for the purpose of changing the label or adding a new indication (Industry Sponsor) • Study results will not be used to change the advertising of the drug (Industry Sponsor) • The investigation does not involve a route of administration or dosage level or use in a patient population or other factor that significantly increases the risks (or decreases the acceptability of risks) associated with use of the drug product (Industry and Academic Sponsors) • The investigation is conducted in compliance with requirements for institutional review • The study will not be used for off-label promotion of the drug (Industry Sponsor) Confidential
Practical Considerations for IND Waivers 17 • Would a change in the route of administration alter the safety profile? • Target Organ may change (i.e. inhaled vs parenteral) • Pharmacokinetics may be altered (i.e. increased renal exposure) • Are the approved doses appropriate for the new indication? • Do animal model data suggest that higher doses should be tested? • Is the intended patient population is within the same age range studied in approved indication • Safety risks in young or older populations may be unknown • Does the intended patient population have a disease condition that would put it at different (i.e., unknown) and/or greater risk than the population studied for the approval (i.e., pediatric versus adult, healthy versus sick) • What were the safety findings for the original indication? • Are those findings relevant for the condition under study? • Don’t short-change the study to avoid an IND • Read the label! Confidential
Investigational Device Exemption(IDE) Waivers • Requirement for IDE based primarily on Device Class (i.e. I, II, or III) • Class III highest risk category • Existence of a “predicate” device • IDE Waivers Based on Risk of Device and Experience with Device Type • Significant Risk (Requires an IDE to initiate a study) • Nonsignificant Risk (May require an IDE) • Exempt (Does not require an IDE)
IDE Exempt Studies • 510(k)-cleared and HDE- or PMA-approved devices, if used in accordance with approved label; • Consumer preference testing of marketed device; • Combinations of legally marketed devices; • Custom devices (NARROWLY defined); • Foreign Studies; Declaration of Helsinki • Studies of diagnostic devices (with some caveats)
Significant Risk Device • Is intended as an implant and presents a potential for serious risk to the health, safety, or welfare of a subject; • Is purported or represented to be for use supporting or sustaining human life and presents a potential for ….; • If for use of substantial importance in diagnosing, curing, mitigating, or treating disease, or otherwise preventing impairment of human health and presents a ….; • Otherwise presents a potential for ….. • Is typically designated as a Class III device
Nonsignificant Risk Devices • An NSR Device is one that does not meet the definition of a Serious Risk Device • Are typically Class I or Class II devices
Who decides whether a device study is SR or NSR? • Study Sponsors make initial determination and present case to IRB • Unless FDA has already determined risk level, it is the responsibility of the IRB to make the determination • FDA is available to consult with sponsor or IRB • In cases of disagreement, FDA trumps IRB
Some Practical Considerations 23 • Plan ahead, evaluate the IND or IDE requirements well before you want to write one • Don’t avoid the FDA – you can save so much time if you ask the questions you need to ask • Read the drug labels, they guide you in determining the information you need to obtain about your own compound • Be thorough in your literature search, the FDA certainly will be • Plan sufficient time to complete the IND or IDE – it can take months to assemble and review all of the data, not days! • Understand import restrictions on clinical supplies and foreign devices • Proofread, proofread, proofread • Poor grammar, sloppy formatting, lack of consistency can impact your working relationship with the FDA • Ask for help – no sense wasting time on rework Confidential
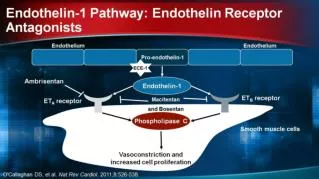
Common IND Misconceptions 24 • The mechanism of action must be well understood prior to submitting an IND for a new drug or biologic drug • Important, but don’t shortchange safety • Use animal models to collect safety information • No safety findings is Good! • Yes, BUT you need to understand the margin of safety between the proposed human dose and the toxic dose • FDA will ask you to find the toxic dose • Regulatory requirements are not relevant to academic research • Early choices can make or break successful translation to industry • Cell line lineage, passage number, viral testing procedures • Antibiotic selection techniques – use of ampicillin not acceptable • Assay reproducibility and accuracy • Regulatory science is not “research” • FDA requirements are science-based • Your grant application is a clinical protocol Confidential
IND/IDE Applications are not Forms • They represent a major scientific effort • Require commitment of time and effort! • They carry a commitment to follow the regulations Confidential
FDA Form 1572 or Investigator Agreement* 26 • Legal Contract between Investigator and Sponsor and FDA • Provides the sponsor with information about the investigator’s qualifications and others at the clinical site • Informs the investigator of his/her obligations and provides the investigator’s written commitment to follow pertinent FDA regulations. • Making a willfully false statement is a criminal offense under 18 U.S.C. 1001. • Submission of a deliberately false statement to the sponsor or to the agency can be taken into consideration in a disqualification proceeding. *for devices Confidential
Statement of Investigator (paraphrased) 27 • Agrees to follow the investigational plan (i.e., the protocol) • Agrees to personally conduct or supervise the conduct of the investigational study and to ensure that all associates, colleagues, understand their obligations to the study • Agrees to inform any study subjects that the drugs /devices are being used for investigational purposes and obtain their consent for participation in the study • Agrees to report adverse experiences that occur in the course of the investigation • Agrees to maintain adequate and accurate records and to make those records available for inspection • Agree to obtain and document IRB approval for the study • Adequately monitor supplies of investigational products used in the study Confidential
Clinical Investigator Inspections 28 • You can expect to be inspected by the FDA if: • You are participating in a Phase 3 industry-sponsored study that will support registration (i.e., approval) of a new drug or biological drug • You are participating in an industry study that will support registration of a new medical device or diagnostic • You are conducting a study funded by the FDA • You are conducting high risk research • A complaint has been lodged against you • You have never been inspected before Confidential
Clinical Investigator Inspection Search FC = for cause; DA = data audit http://www.accessdata.fda.gov/scripts/cder/CLIIL/index.cfm?fuseaction=Search.Search
FDA Inspection Codes Classification Codes Frequency of Classification in Washington State Inspections NAI – 27% VAI – 69.5% OAI – 1% CANC – 1.5% WASH – 0.5% • NAI – No Action Indicated • VAI – Voluntary Action Indicated • OAI – Official Action Indicated • CANC – Cancelled • WASH – Washout
Errors Frequently Committed by Clinical Investigators in Washington State
ITHS Preclinical Research and Development Core 32 • Consulting on IND/IDE Content • Preparation of IND/IDE • Review Development Programs • Assist in identification of industry and academic partners • Funding Program for Translational Research (Ignition Awards for Nonhuman Primate studies, Pharmaceutics, and Manufacturing) • (ithsprdn@u.washington.edu)
Thank you For additional information contact:Lynn Rose 206-884-7540
Objectives • Provide an overview of: • How to assess study feasibility • Clinical research approval process- UW • Where you can go for help
Study feasibility • Population • Procedures • Collaborations • Staff • Budget • Space • etc.
Population • Do you have access to the right patient population? • Are the enrollment goals realistic? • Will you need to recruit outside of your system? • Will enrollment compete with other studies? • Are there special consent issues? • Have you reviewed the inclusion/exclusion criteria and are they too restrictive?
Procedures • Are procedures approvable? • Are procedures frequent/painful/inconvenient? • Do procedures require special equipment/expertise?
Collaborations • Do you need additional specialists? • Do you need access to outside clinics/schools/etc?
Personnel • Do you have qualified staff? • Any special training required? • Do you need an RN? • Do you have time to devote to the protocol? • Does your staff have time to devote to the protocol?
Budget Considerations • Your time • Staff time • Sub-investigator time • Consultant time • Cost of procedures • Cost of labs • Cost of space (CRC) • Cost of shipping • Records Storage • Cost of storing specimens • Pharmacy costs • Cost of data collection system • Cost of monitoring (study and site) • Cost of statistician • Manuscript preparation and presentation
Budgets • If budget is determined by sponsor do they allow time for • Study start-up activities (non-refundable) • Training • Unanticipated activities – protocol amendments, unanticipated monitoring visits, audits, etc • Keep in mind industry budgets are negotiable • If you are writing the budget, is the RFA amount sufficient for all the study activities? • If not – what will need to be cut from the protocol.
Budgeting help • CRBB Detailed Budget Tool • https://depts.washington.edu/crbb/Submit_Budget.shtml • For help contact CRBB • CRBB@uw.edu • 206-543-7774
Space • Do you have room for: • Research personnel • Study binders • Any equipment needed • Lab supplies OR • Will you have to look for more space?
Start up activities - contracts • Read the protocol • Make sure everyone on the research team reads the protocol • Decide if the study is feasible • Let your Division/Departmental administrator know you are thinking of pursuing/accepting the contract
Considerations if you didn’t write the protocol • Is it well designed? • Any ethical issues? • Is there potential benefit to participants? • Will the sponsor allow modifications if you don’t think it is feasible as written? • Are the visits/procedures onerous for participants? • Drug available at the end of the study?
Study start-up activities - Develop all study materials • Regulatory Binder • Study visit records • Case report forms • Eligibility checklist • Adverse event report forms • Protocol deviation report forms • Screening logs • Training logs • PI Delegation log ITHS forms - www.iths.org/forms https://www.washington.edu/research/clinical-research-handbook//
Study start up activities – training • Human Subjects Protection • Good Clinical Practice • HIPAA • Clinical Research Budget and Billing • Office of Sponsored Research seminars • Clinical Research Education Series – ITHS • Fundamentals of Clinical Research - ITHS
Who to go to for help • General questions about clinical research at the UW – Ella Mae Kurashige, Director Clinical Research Services - ellamaek@uw.edu • Office of Sponsored Programs - http://www.washington.edu/research/osp/?page=osp • ITHS Research Navigator - https://www.iths.org/help • UW Clinical trials handbook https://www.washington.edu/research/clinical-research-handbook//: submission checklists, repository for how to do clinical research at the UW Medicine
Who to go to for help • How to get assistance from a research coordinator – Michelle Doyle – ITHS Research Coordinator Core rccore@uw.edu • Study design and biostatistical help – ITHS Center for Biomedical Statistics http://depts.washington.edu/medstat/Welcome.html • Investigational Drug Service – Sheree Miller – uwmcids@uw.edu • Research Bioethics – Ben Wilfond - ITHS RSB core rsbcore@u.washington.edu