Download
1 / 15
160 likes | 280 Views
Past Experiences and Workshop Goals. Khoti Gausi gausik@zw.afro.who.int Monitoring and Evaluation WHO Inter-Country Support Team for Malaria in East and Southern Africa. RBM and Abuja.

E N D
Past Experiences and Workshop Goals Khoti Gausi gausik@zw.afro.who.int Monitoring and Evaluation WHO Inter-Country Support Team for Malaria in East and Southern Africa RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia
RBM and Abuja • RBM and Abuja 2000 goals - to reduce morbidity and mortality due to malaria by 50% (base year 2000) by 2010. • Intermediate targets for end of 2005: 60% coverage of malaria control interventions for U5s and pregnant women. • But in 2006 Abuja Summit in May and concluded with Abuja Call = universal access to malaria control interventions. RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia
Measurement of progress • Need for showing progress on coverage of interventions and impact on the disease. • Interventions = community surveys • Impact on the disease = routine data (health facility) and community surveys • In fact, initially, any methodology (academic or not) was OK, so long we got some figure until RBM technical partners got involved in MIS. RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia
RBM and Abuja • RBM survey tools around 2000 and 2001 for baseline. Mostly focused in “RBM districts” (a few districts). Sampling based on health facility sampling. Thus this was an IMCI (health facility) survey conveniently collecting some community data for malaria. • DHS and MICS remained as reference population based surveys. RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia
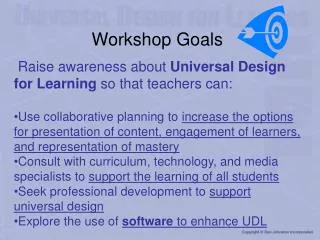
RBM Districts in Southern Africa The RBM districts represent themselves only. If you take a representative sample of households in the districts they do not represent the situation in the country. RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia
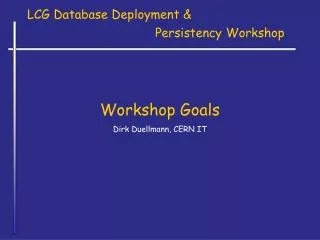
U5 ITN use in Malawi collected by various tools RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia
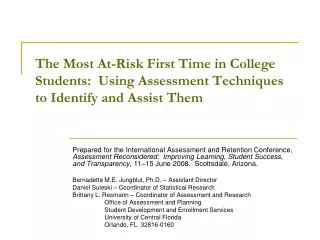
U5 ITN use in Zambia by various tools RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia
Back to the Tools • How about you in your country? • Do you find the same situation in your country? • Tell us about it. RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia
RBM produces the MIS • DHS and MICS done during the low malaria seasons for logistical ease. • They sample from all districts in the country regardless of their malaria situation. • In a country where malaria is epidemic then missing the season may purely take malaria out of the survey. • Thus partners looking for a tool that is combines characteristics of DHS and MICS and incorporates malaria concerns. RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia
Experiences with MIS • First MIS was done in Zambia in 2006. • Then Angola, Mozambique, Kenya, Ethiopia, Zimbabwe, ... Other countries have also done sub-national MIS. • In each country some challenges were common to all countries, some were country specific. RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia
Issues • Sampling: is based on morbidity, not mortality. Thus sample is lower than in DHS, etc. • Need to involve central statistics offices. • Use of PDAs enriches the data collected. Paper makes the work much harder. • Planning in advance is critical. • The MIS costs money. Lesson and reminder: quality data is not cheap. RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia
Issues (2) • Can produce results more quickly than DHS or MICS. • Collects both coverage and impact data. • When using PDAs programming capacity is lacking. • Even though TA is available from (a few) partners there is need fro strong leadership from the NMCP to have a successful MIS. • What are the other issues that you would include? (for countries who have already done a MIS) RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia
Workshop Objective Build capacity in planning and conducting a Malaria Indicator Survey (MIS) in Anglophone Africa. RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia
Specific Objectives Review and discuss • planning of an MIS • questionnaires and data collection tools – PDAs and paper • parasitemia and anaemia testing • training of enumerators and supervisors and data collection and field operations • supervision and troubleshooting • Data entry, cleaning and analysis; report writing and dissemination RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia
Past Experiences and Workshop Goals Khoti Gausi gausik@zw.afro.who.int Monitoring and Evaluation WHO Inter-Country Support Team for Malaria in East and Southern Africa RBM-MERG Malaria Indicator Training Workshop, 9th-12th September 2008, Lusaka, Zambia