Download
1 / 17
170 likes | 269 Views
Back and Pelvis. Lab 4 Case Study #2 Group #6. Introduction Case Study Client. 30 year old female (4 weeks post natal) Experiences pain in her SI region during walking gait, sitting, standing, sleeping Difficulty with lifting

E N D
Back and Pelvis Lab 4 Case Study #2 Group #6
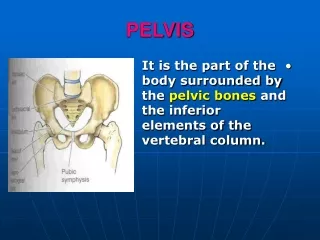
IntroductionCase Study Client • 30 year old female (4 weeks post natal) • Experiences pain in her SI region during walking gait, sitting, standing, sleeping • Difficulty with lifting • Previously treated for sacral displacement and pelvic re-alignment for last 4 weeks • Regained range through passive walking program and anti inflammatory drugs • Client is a pronator with knee problems due to foot malfunction • Client has medium lumbar lordosis and slight scoliotic spine • Client experienced low back pain prior to pregnancy, however not SI joint related
General ScanStanding Forward Bend Test • Patient stands with feet shoulder width apart • Clinician faces patients back, places thumbs on patients PSIS and hands on iliac crest • Clinician instructs patient to bend forward • If SI joint is normal, clinicians thumbs will move inferiorly as patient bends forward • If lesion is present, thumb on affected side will either move upward or not move at all • Test identifies side of lesion, however does not identify type of lesion
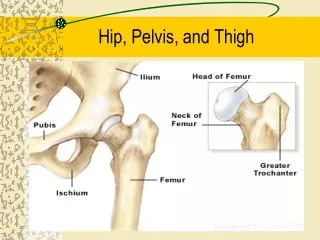
Possible Limitations • Possible limitations that could affect movement of the pelvic region include damage to: • sacrotuberous, sacroiliac, and sacrospinous ligaments • Muslces that could limit movement of the pelvic region include: • Hip flexors (ilio psoas, rectus femoris), hip extensors (gluteus maximus, biceps femoris)
General ScanLeg Length Difference Test • Clinicians instructs patient to lie supine on table with patient’s arms by their side • Clinician instructs patient to flex both legs at hips and knees then move legs to full extension in supine position • Clinician lightly shakes patient’s legs at feet to ensure relaxation of patient • Clinician observes spine of patient to see if spine is perpendicular to ASIS • Clinician places both medial malleoli’s together and takes note of differences in leg length • *A leg length discrepancy does not necessarily entail that the patient has a lesion in their SI joint. This test should be used in conjuction with other SI tests to ensure complete accuracy
General ScanKinetic Test • Patient stands with her back to clinician • To evaluate the left side of patient, the clinician places one thumb on the patients left PSIS and other thumb on the mid sacrum of the same side • The clinician instructs the patient to lift her left knee toward her chest • If the SI is normal the clinicians left thumb on affected side will move inferiorly • If a lesion is present, clinicians left thumb will stay at same point or move superiorly • Clinician then tests patient’s right side by instructing patient to flex right leg while their hands remain in their original position • Clinician then repeats the same test on the right side with their thumb on patient’s right PSIS and other thumb on the mid sacrum same side
Thomas Test • Part 1(PROM) • Patient lies supine on examination table • Spine is square to ASIS • Clinician stabilizes patient’s back by supporting lumbar spine with hand • Clinician flexes a leg up towards patient’s chest • Note when lumbar lordosis flattens and the patients back touches your hand • Once lordosis is flattened continue flexion at hip until end point • *120 degrees is normal • Goniometer is used to measure and record range of motion at hip • Repeat on other side
Thomas Test Con’t • Part 2 (AROM) • Patient holds one leg up by their chest while extending their other leg • Watch for the patient rocking forward/lifting of the thoracic spine or arching/reformation of the lumbar lordosis • Either rocking or arching of the back are evidence that the patient has a contracture • Extent of the contracture can be measured as the angle created between the leg and table • Repeat for the other side
Functional Test 1)Lifting box from different levels a) Lift box off chair on to table: • To begin patient stands close to table • Patient then moves farther away from table when they feel more comfortable • One foot slightly in front of the other and feet are shoulder width apart for balance • Lifting is done with legs not back (flex at knees) b) Lift box from floor to table: • Repeat the steps mentioned above
Functional Test Con’t 2)Sit and tie shoes then stand up: • Patient starts standing then moves to a seated position • Patient then leans forward to tie shoes on one foot, then ties shoes on other foot • Next patient stands up • Clinician watches if patient: • Uses hands to get off chair • Rocks back and forth for momentum • Adjusts leg width or pushes off with toes of non-tying foot • Wraps leg around chair
References • Hoppenfield, JA (1934). Physical Examination of Spine and Extremities. New York : Appleton-Century-Crofts. • Houglum, Peggy A. (n.d.). Therapeutic Exercise for Musculoskeletal Injuries, 2nd ed. • Oatis, Carol A. (2004). Kinesiology: The Mechanics & Pathomechanics of Human Movement. Pennsylvania: Lippincott, Williams & Wilkins