Download
1 / 32
340 likes | 860 Views
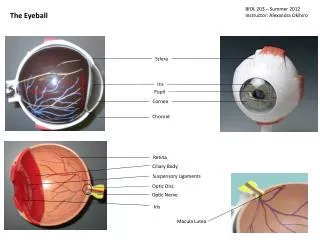
Episclera and sclera. Dr. Mohammad Shehadeh. Anatomy. The three vascular layers that cover the anterior sclera are: The conjunctival vessels are the most superficial; arteries are tortuous and veins straight.

E N D
Episclera and sclera Dr. Mohammad Shehadeh
Anatomy • The three vascular layers that cover the anterior sclera are: • The conjunctival vessels are the most superficial; arteries are tortuous and veins straight. • The superficial episcleral plexus vessels are straight with a radial configuration. In episcleritis, maximal congestion occurs within this vascular plexus (Fig. 8.1A). Tenon capsule and the episclera are infiltrated with inflammatory cells, but the sclera itself is not swollen. Instillation of topical phenylephrine will cause blanching of the conjunctival and to a certain extent the superficial episcleral vessels, allowing visualization of the underlying sclera. • The deep vascular plexus lies in the superficial part of the sclera and shows maximal congestion in scleritis (Fig. 8.1B). There is also inevitably some engorgement of the superficial vessels, but this should be ignored. Examination in daylight is important to localize the level of maximal injection; scleritis often has a purplish hue.
Episcleritis • Episcleritis is a common, benign, usually idiopathic, recurrent and frequently bilateral condition. It is usually self-limiting and an attack typically lasts a few days
Signs • Presentation is with redness and mild discomfort. • Redness may be sectoral or diffuse. Often it has an interpalpebral distribution, in contrast with scleral disease which commonly starts in the upper temporal quadrants. • The attack often reaches its peak within 12 hours and then gradually fades over the next few days. • The episcleritis often flits from one eye to the other or may be bilateral.
Treatment • If mild, no treatment is required • Cool artificial tears may be adequate in some cases. • A weak topical steroid q.i.d. for 1–2 weeks is usually sufficient, though occassionally more intensive instillation is needed initially. • Oral NSAIDs are sometimes required such as flurbiprofen 100 mg t.i.d. for 10 days.
Nodular episcleritis • Nodular episcleritis also tends to affect young females but has a less acute onset and a more prolonged course than the simple variety • One or more tender nodules, almost always within the interpalpebralfissure • A thin slit-lamp section shows that the anterior scleral surface is flat, indicating absence of scleral involvement
Instillation of 2.5% phenylephrine drops will decongest the conjunctival and episcleral vessels allowing better visualization of underlying sclera. • Each attack is self-limiting and usually clears without treatment but tends to last longer than simple episcleritis. • After several attacks the vessels surrounding the inflamed area may become permanently dilated. • It is important to exclude a local cause for an episcleral nodule such as a foreign body or granuloma.
Immune-mediated scleritis • Classification of immune-mediated scleritis Anterior • Non-necrotizing • Diffuse • Nodular • Necrotizing with inflammation • Vaso-occlusive • Granulomatous • Surgically-induced • Scleromalaciaperforans • Posterior
Anterior non-necrotizing scleritis • Diffuse: • Diffuse disease is slightly more common in females and usually presents in the 5th decade. • usually with ocular redness followed a few days later by aching and pain which may spread to the face and temple. • The pain typically wakes the patient in the early hours of the morning and improves later in the day; it responds poorly to common analgesics
SIGNS • Vascular congestion and dilatation associated with oedema. • The redness may be generalized or localized to one quadrant • As the oedema resolves, the affected area often takes on a slight grey/blue appearance because of increased scleral translucency; this is due to rearrangement of scleralfibres rather than a decrease in scleralthickness • Recurrences at the same location are common unless the underlying cause is treated.
Nodular • Presentation is with the insidious onset of pain followed by increasing redness, tenderness of the globe and the appearance of a scleralnodule • Slit-lamp examination shows that the slit beam is displaced by the scleral nodule (Fig. 8.5B). • Instillation of 2.5% phenylephrine drops will constrict the conjunctival and superficial episcleral vasculature but not the deep plexus over the nodule.
Anterior necrotizing scleritis with inflammation • Necrotizing disease is the aggressive form of scleritis. • The age at onset is later than that of non-necrotizing scleritis, averaging 60 years. • The condition is bilateral in 60% of patients and unless appropriately treated, especially in its early stages, it may result in severe visual morbidity and sometimes loss of the eye.
Signs • Presentation is with gradual onset of pain which becomes severe and persistent and radiates to the temple, brow or jaw; it frequently interferes with sleep and responds poorly to analgesia.
Types • Vaso-occlusive is often associated with rheumatoid arthritis. • Granulomatous is often associated with Wegener granulomatosis and polyarteritisnodosa • Surgically-induced scleritis typically starts within 3 weeks of the surgical procedure
Complications • Acute infiltrative stromalkeratitis • Sclerosing keratitis, the peripheral cornea adjacent to the site of scleritis resembles sclera • Peripheral ulcerative keratitis is characterized by progressive melting and ulceration which may eventually be more serious than the scleritis. • Uveitis, if severe, usually denotes aggressive scleritis. • Glaucoma • Hypotony may be the result of ciliary body detachment, inflammatory damage or ischaemia. • Perforation of the sclera as a result of the inflammatory process alone is extremely rare.
Scleromalaciaperforans • Scleromalaciaperforans is a specific type of necrotizing scleritis without inflammation that typically affects elderly women with longstanding rheumatoid arthritis
Signs • Presentation : is with slight non-specific irritation, pain is absent and vision unaffected. • Necrotic scleral plaques near the limbus without vascular congestion • Very slow progression of scleral thinning and exposure of underlying uvea (Fig. 8.10B).
Posterior scleritis • Posterior scleritis is a serious, potentially blinding condition, which is often misdiagnosed and treated very late. • The age at onset is often under the age of 40 years. • The disease is bilateral in 35% of cases. • Young patients are usually healthy but about a third of those over the age of 55 years have associated systemic disease.
Signs • Presentation may be with discomfort or pain • Exudative retinal detachment occurs in almost 25% of cases • Uvealeffusion characterized by exudative retinal detachment and choroidal detachment • Choroidalfolds • Subretinal mass characterized by a yellowish-brown elevation which may be mistaken for a choroidaltumour. • Disc oedema with an accompanying slight reduction of vision is common. • Myositis is common and gives rise to diplopia, pain on eye movement, tenderness to touch and redness around a muscle insertion. • Proptosis is usually mild and frequently associated with ptosis.
Ultrasound: • Fluid in Tenon's space gives rise to the characteristic ‘T’ sign in which the stem of the T is formed by the optic nerve on its side and the cross bar by the gap containing fluid
Treatment of immune-mediated scleritis 1 Topical steroids do not affect the natural history of the scleral inflammation, but may relieve symptoms and oedema in non-necrotizing disease. 2 Systemic NSAIDs should be used only in non-necrotizing disease. 3 Periocularsteroid injections may be used in non-necrotizing and necrotizing disease but their effects are usually transient. 4 Systemic steroids are used when NSAIDs are inappropriate or ineffective (necrotizing disease). 5 Cytotoxicagents are usually necessary whenever disease activity is not completely controlled with steroids alone, or as a steroid-sparing measure in patients requiring long-term treatment. 6 Immune modulators such as ciclosporin and tacrolimus are less useful as long-term therapy