Download
1 / 1
30 likes | 508 Views
O. Della Gatta (*), C. Guarino (**), G. Iepparelli (**), A. Turco (***),C. Cesaro (***), G. La Cerra (***), D. Della Gatta (***). (*) U.O.C. Anestesia e Terapia Intensiva - A.O.R.N. Monaldi – Dir. A. Corcione

E N D
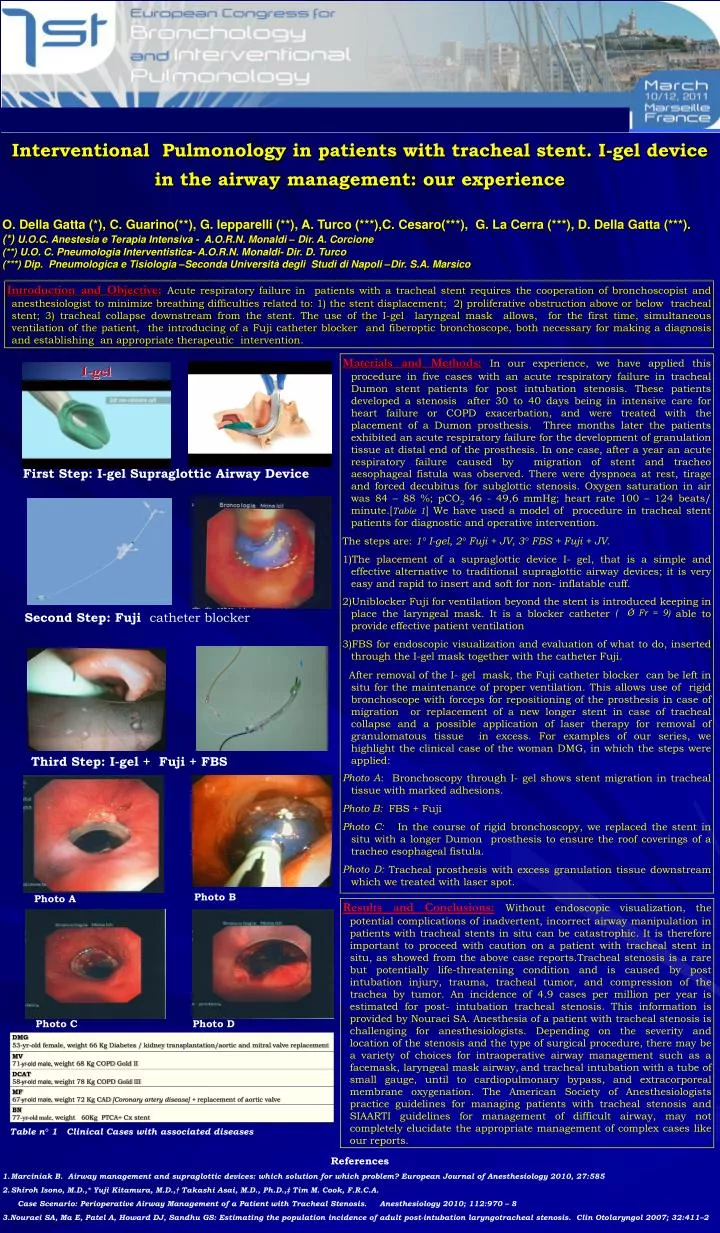
O. Della Gatta (*), C. Guarino(**), G. Iepparelli (**), A. Turco (***),C. Cesaro(***), G. La Cerra (***), D. Della Gatta (***). (*) U.O.C. Anestesia e Terapia Intensiva - A.O.R.N.Monaldi – Dir. A. Corcione (**) U.O. C. Pneumologia Interventistica- A.O.R.N.Monaldi- Dir. D. Turco (***) Dip. Pneumologica e Tisiologia –Seconda Università degli Studi di Napoli –Dir. S.A. Marsico Introduction and Objective:Acute respiratory failure in patients with a tracheal stent requires the cooperation of bronchoscopist and anesthesiologist to minimize breathing difficulties related to: 1) the stent displacement; 2) proliferative obstruction above or below tracheal stent; 3) tracheal collapse downstream from the stent. The use of the I-gel laryngeal mask allows, for the first time, simultaneous ventilation of the patient, the introducing of a Fuji catheter blocker and fiberoptic bronchoscope, both necessary for making a diagnosis and establishingan appropriate therapeuticintervention. Interventional Pulmonology in patients with tracheal stent. I-gel device in the airway management: our experience • Materials and Methods:In our experience, we have applied this procedure in five cases with an acute respiratory failure in tracheal Dumon stent patients for post intubation stenosis. Thesepatientsdeveloped a stenosisafter 30 to 40 daysbeing in intensive care forheartfailure or COPD exacerbation, and weretreatedwith the placementof a Dumonprosthesis. Three monthslater the patientsexhibitedan acute respiratoryfailurefor the developmentofgranulationtissue at distal end of the prosthesis. In one case, after a yearan acute respiratoryfailurecausedbymigrationofstent and tracheoaesophagealfistulawasobserved. There were dyspnoea at rest, tirage and forced decubitus for subglotticstenosis. Oxygen saturation in air was 84 – 88 %; pCO2 46 - 49,6 mmHg; heart rate 100 – 124 beats/ minute.[Table 1]We have used a model of procedure in tracheal stent patients fordiagnostic and operative intervention. • The steps are: 1° I-gel, 2° Fuji + JV, 3° FBS + Fuji + JV. • The placementof a supraglotticdeviceI- gel, that is a simple and effective alternative to traditional supraglottic airway devices; it is very easy and rapid to insert and soft for non- inflatable cuff. • Uniblocker Fuji for ventilation beyond the stentisintroducedkeeping in place the laryngealmask. Itis a blockercatheter( Ǿ Fr = 9)abletoprovideeffectivepatientventilation • FBS for endoscopic visualization and evaluation of what to do, insertedthrough the I-gelmasktogetherwith the catheter Fuji. • Afterremovalof the I- gel mask, the Fuji catheterblocker can beleft in situ for the maintenanceofproperventilation. Thisallowsuseofrigidbronchoscopewithforcepsforrepositioningof the prosthesis in case ofmigration or replacementof a newlongerstent in case oftrachealcollapse and a possibleapplicationof laser therapyforremovalofgranulomatoustissue in excess.Forexamplesofourseries, wehighlight the clinical case of the woman DMG, in which the stepswereapplied: • Photo A: Bronchoscopythrough I- gel showsstentmigration in trachealtissuewithmarkedadhesions. • Photo B: FBS + Fuji • Photo C: In the courseofrigidbronchoscopy, wereplaced the stent in situ with a longerDumonprosthesistoensure the roofcoveringsof a tracheoesophagealfistula. • Photo D:Trachealprosthesiswithexcessgranulationtissue downstream whichwetreatedwith laser spot. First Step: I-gelSupraglotticAirwayDevice SecondStep: Fuji catheter blocker Third Step: I-gel + Fuji + FBS Photo B Photo A Results and Conclusions:Without endoscopic visualization, the potential complications of inadvertent, incorrect airway manipulation in patients with tracheal stents in situ can be catastrophic. It is therefore important to proceed with caution on a patient with tracheal stent in situ, as showed from the above case reports.Tracheal stenosis is a rare but potentially life-threatening condition and is caused by post intubation injury, trauma, tracheal tumor, and compression of the trachea by tumor. An incidence of 4.9 cases per million per year is estimated for post- intubation tracheal stenosis. This information is provided by Nouraei SA. Anesthesia of a patient with tracheal stenosis is challenging for anesthesiologists. Depending on the severity and location of the stenosis and the type of surgical procedure, there may be a variety of choices for intraoperative airway management such as a facemask, laryngeal mask airway,and tracheal intubation with a tube of small gauge, until to cardiopulmonary bypass, and extracorporeal membrane oxygenation. The American Society of Anesthesiologists practice guidelines for managing patients with tracheal stenosis and SIAARTI guidelines for management of difficult airway, may not completely elucidate the appropriate management of complex cases like our reports. Photo C Photo D Table n° 1 Clinical Cases withassociated diseases • References • Marciniak B. Airway management and supraglottic devices: which solution for which problem? European Journal of Anesthesiology 2010, 27:585 • ShirohIsono, M.D.,* Yuji Kitamura, M.D.,† Takashi Asai, M.D., Ph.D.,‡ Tim M. Cook, F.R.C.A. • Case Scenario: Perioperative Airway Management of a Patient with Tracheal Stenosis. Anesthesiology 2010; 112:970 – 8 • 3.Nouraei SA, Ma E, Patel A, Howard DJ, Sandhu GS: Estimating the population incidence of adult post-intubation laryngotrachealstenosis. ClinOtolaryngol 2007; 32:411–2