Download
1 / 15
150 likes | 294 Views
Infant Survival: Meeting the Challenges of Maternal-Child HIV. Doug Watson MD (Robb Sheneberger MD) University of Maryland, School of Medicine Institute of Human Virology Monday August 11 Sixth Annual Tract I Meeting. AIDSRelief Tanzania Challenges.

E N D
Infant Survival:Meeting the Challenges of Maternal-Child HIV Doug Watson MD (Robb Sheneberger MD) University of Maryland, School of Medicine Institute of Human Virology Monday August 11 Sixth Annual Tract I Meeting
AIDSRelief Tanzania Challenges • Only 56% of women who were first seen in either ANC (99% tested) or L&D (28% tested)received HIV CT (but 60% of women were first seen in L&D) • Only 47% of known positives received any ARV, and 95% of those getting any ARV prophylaxis received only sd-NVP
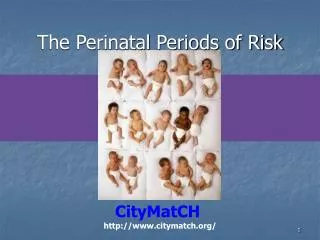
Age Range of Children on ART 536 total charts reviewed. Overall median age for population was 6.5 years
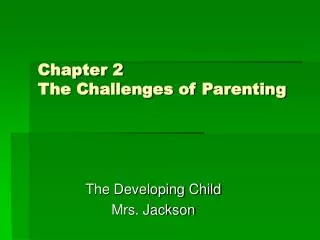
Proportion of Patients VL <200c/mm3 N=466 N=536 85.4% On Treatment 74.2% ITT (missing=failure) Same country adult suppression on treatment 94.6%
Regimen Choice and Suppression p<.001 Children on a Lop/r containing 1st regimen were 11.69 times (Pearson Chi2 = 11.6954) more likely to be suppressed at review than patients on 1st regimen that did not contain Lop/r
NVP and Suppression p<.0001 Children on a NVP containing 1st regimen were 17.98 times (Pearson Chi2 = 17.9804) more likely to have viral failure at review than patients on 1st regimen that did not contain NVP
Common Problems with Care of Infected Children • Where are they? Average age at ART initiation is 6.5 years meaningmost die before diagnosis and treatment • Delay in infant diagnosis • Unavailability or tardiness of DNA PCR • Lack of understanding of clinical diagnosis- developmental milestones and growth curves • ART guidelines that do not recommend treatment of children at high risk of progression (initiating treatment at much too advanced disease in children)
Common Problems with Care of Infected Children • Use of NVP-based regimen in children exposed to NVP • Dosing errors (under dosing) • Need for child-specific approach to care & adherence • Not recognizing treatment failure • Limited options after prolonged initial thymidine based regimen failure
Problem: Opportunities to reduce morbidity and mortality in HIV-infected and –affected children are being missed. Response: University of Maryland/IHV AIDSRelief integrated Maternal-Child HIV care strategy
Minimize transmission from mother to child • Establish community-based identification of infected pregnant women • Engage pregnant women into comprehensive HIV care system • A maternal-child focused approach within a comprehensive HIV care system rather than a vertically-integrated “PMTCT” program • Earlier and more aggressive ART for pregnant women • ARV prophylaxis to protect breastfeeding infants • Data on maternal HAART more mature at this point than ARV prophylaxis to infant
Provide a package of support for HIV-exposed infants • Enroll infected pregnant women and exposed infants in AR program and provide package of care until 2 years of age • Infant nutrition counseling • Starting in antenatal period and continuing through infancy • More evidence-based: Base counseling on risk of HIV infection or death from substitute feeding for the individual infant • Facilitate general availability of robust early infant virologic diagnosis • Emphasize clinical diagnosis in interim
Rapidly diagnose infants and children • Facilitate general availability of robust early infant virologic diagnosis • Training on importance of early diagnosis of infants and children • Broad testing of children: every child should have his HIV-exposure or HIV-infection status determined • Multiple entry points: Children and siblings of patients, child health center attendees, in-patients, orphanages, community-based testing, etc.
Ensure long-term health of infected children • Evidence-based, non-discriminatory identification of children who require ART • Many current guidelines do not treat children at much higher risk of progression than adult guidelines allow • Selection of regimens that maximize prospect for long-term viral suppression with minimal toxicity • NVP based regimens with high viral loads and after sd-NVP exposure inadequate • Failure of current standard thymidine regimens leaves few options • Child-focused clinical services
Engage mothers and families in HIV care • Testing of children & partners of infected women • The best OVC strategy is to prevent Vulnerable Children from becoming Orphans • Family-based tracking • Family clinic: parents and children seen at same time • Engagement of parents in care, particularly fathers
Measure meaningful outcomes applied across the community • Use ANC seroprevalence and census data to estimate proportion of infected pregnant women who engage in care in communities served by AR • Monitoring maternal-child care “cascade” on site-specific basis to identify system gaps • Link mothers and children • Determine final infection status • Determine infant survival (12 months) and at 18 & 24 months • Pediatric targeted evaluation of viral suppression • Use outcomes data to advance program