Download
1 / 77
791 likes | 1.21k Views
VOGT-KOYANAGI-HARADA DISEASE. AHMED M. ABU EL-ASRAR, MD, PhD. Department of Ophthalmology, College of Medicine, King Saud University, Riyadh, Saudi Arabia Dr. Nasser Al-Rashid Research Chair in Ophthalmology. VKH Disease. Multisystem disease

E N D
VOGT-KOYANAGI-HARADADISEASE AHMED M. ABU EL-ASRAR, MD, PhD Department of Ophthalmology, College of Medicine, King Saud University, Riyadh, Saudi Arabia Dr. Nasser Al-Rashid Research Chair in Ophthalmology
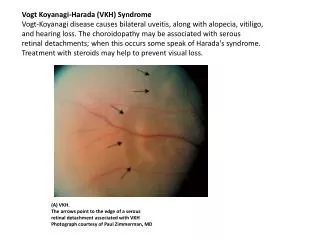
VKH Disease • Multisystem disease • Chronic, bilateral, granulomatous panuveitis associated with central nervous system, auditory and integumentary manifestations Moorthy et al: SurvOphthalmol 1995; 39:265 (review) Read et al: Am J Ophthalmol 2001;131:647
VKH Disease Epidemiology • Individuals with a predisposing genetic background. • Ethnic groups with more heavily pigmented skin. • Asians, Native Americans, Hispanics, Asian Indians, Middle Easterners.
VKH Disease Epidemiology • Genetic background rather than degree of skin pigmentation. • Women more than men. • 3rd – 4th decade. • Pediatric age group. Read et al: CurrOpinOphthalmol 2000;11:437 (review) Abu El-Asrar et al: Eye 2008;22:1124 Martin et al: Retina 2010 Feb 17. [Epub ahead of print]
VKH Disease Etiology and Pathogenesis • Remains unknown. • T-lymphocyte mediated autoimmunity directed against one or more antigens found on or associated with melanocytes found in eye, skin and hair, inner ear, CNS. Okada et al: Graefe’s Arch Clin Exp Ophthalmol 1996;234:359
VKH Disease Etiology and Pathogenesis • Tyrosinase family proteins are enzymes for melanin formation and are expressed in melanocytes. • T-lymphocytes from VKH disease patients proliferate in response to tyrosinase, TRP1 or TRP2. • Immunization of Lewis rats with tyrosinase, TRP1 or TRP2 produced an inflammatory disease that resembled VKH disease with skin lesions and meningitis. Yamaki et al: J Immunol 2000;165:7323 Yamaki et al: Exp Eye Res 2000;71:361
VKH Disease Etiology and Pathogenesis • Th cells from peripheral blood of VKH patients produce predominantly Th1 cytokines (IFN-gamma, IL-2) especially when stimulated • T-cell clones specific to tyrosinase family proteins established from peripheral blood mononuclear cells of patients with VKH disease showed proliferative responses to tyrosinase and/or TRP1 and produced Th1-type cytokines. Imai et al: Curr Eye Res 2001;22:312 Gocho et al: Invest Ophthalmol Vis Sci 2001;42:2004
VKH Disease Etiology and Pathogenesis • IL-23 stimulated production of IL-17 by CD4+ T cells may be responsible for the development of VKH disease. Fang and Yang: Curr Eye Res 2008;33:517
VKH Disease Etiology and Pathogenesis • VKH-like disease in patients treated with interferon-alpha and ribavirin therapy for chronic hepatitis C virus infection. Al-Muammar et al: IntOphthalmol 2010 Feb 23. [Epub ahead of print] Sene et al: World J Gastroenterol 2007;13:3137 Touitou et al: Am J Ophthalmol 2005;140:949 Papastathopoulos et al: J Infect 2006;52:e59 Kasahara et al: J Gastroenterol 2004;39:1106 Sylvestre et al: J Viral Hepat 2003;10:467
VKH Disease Pathology • Granulomatous panuveitis. • Lymphocytes, epitheloid cells, few plasma cells, multinucleated giant cells. • Epitheloid cells and giant cells contain melanin pigment.
VKH Disease Pathology • Dalen-Fuchs’ nodules: Lymphocytes, epitheloid cells, pigment-laden macrophages, altered and/or proliferated RPE cells. • Melanocytes disappear from choroid. Perry and Font: Am J Ophthalmol 1977;83:242 Inomata and Rao: Am J Ophthalmol 2001;131:607
VKH Disease Genetic Factors • Certain racial groups. • Immunogenetic predisposition. • Strong association with HLA-DR4 and HLA-DRw53 with the most significant risk allele being HLA-DRB1*0405. • Causative pathogenic antigen binds with HLA-DRB1*0405 molecule which presents the antigen to T cells to activate them. Fang and Wang: Curr Eye Res 2008;33:517 (review). Read et al: CurrOpinOphthalmol 2000;11:437 (review). Yamaki et al: IntOphthalmolClin 2002;42:13 (review).
VKH Disease Genetic Factors • VKH disease in monozygotic twins • Familial VKH disease • Familial cases shared HLA-DR4 Itho et al: IntOphthalmol 1992;16:49 Rutzen et al: Am J Ophthalmol 1995;119:239 Sonoda et al: Jpn J Ophthalmol 1999;43:113
VKH Disease Clinical FeaturesExtraocular Manifestations Integumentary Manifestations • Sensitivity of hair and skin to touch (early in prodromal phase). • Poliosis, vitiligo, alopecia (during convalescent stage). • Ethnic groups may manifest varying systemic symptoms.
VKH Disease Clinical FeaturesExtraocular Manifestations Neurologic Manifestations • Most common during prodromal stage. • Neck stiffness, headache, confusion. • Occasionally focal neurologic signs. • CSF pleocytosis.
VKH Disease Clinical FeaturesExtraocular Manifestations Auditory Manifestations • May be presenting problem • Sensorineural hearing loss usually involves higher frequencies • Tinnitus • Vertigo • May cause permanent hearing loss
VKH Disease Clinical FeaturesAuditory Manifestations
VKH Disease Clinical Course 4 phases • Prodromal • Acute uveitic • Convalescent or chronic • Chronic recurrent
VKH Disease Clinical Course Prodromal Phase: • Mimics viral illness • Neurologic and auditory manifestations • Few days • Headache, orbital pain, stiff neck, malaise, abdominal pain, nausea, fever, vertigo, tinnitus • Cranial nerve palsies, optic neuritis (rare) • CSF pleocytosis
VKH Disease Clinical Course Acute Uveitic Phase: • Bilateral in 70% of patients, delay of 1-3 days before 2nd eye becomes involved in 30%. In a few cases this interval may last up to 10 days. • Hallmark is bilateral multifocal exudative retinal detachments, hyperemia and edema of the optic disc.
VKH Disease Clinical Course Acute Uveitic Phase: (cont.). • Yellow-white lesions at level of RPE beneath serous RD. • Thickening of posterior choroid manifested by elevation of peripapillary retino-choroid layer. • Retinal edema in posterior pole. • Peripheral well-circumscribed yellow-white lesions (clinical equivalent of Dalen-Fuchs’ nodules).
VKH Disease Clinical Course Acute Uveitic Phase: (cont.) • No inflammation of the anterior segment or mild to moderate nongranulomatous anterior uveitis if the disease is not well controlled with appropriate treatment during the first two weeks. Fang and Yang: Curr Eye Res 2008;33:517 (review)
VKH Disease Clinical Course Acute Uveitic Phase: (cont.). • Shallow anterior chamber • Elevated IOP • Acute angle closure glaucoma
VKH Disease Clinical Course Convalescent Phase: • Integumentary and uvea depigmentation. • Perilimbal vitiligo (Sugiura’s sign). • Fundus exhibits an orange-red discoloration (“sunset-glow” fundus).
VKH Disease Clinical Course Convalescent Phase: (cont.) • Multiple small yellow well-circumscribed areas of chorioretinal atrophy representing regressed Dalen-Fuchs’ nodules. • RPE clumping or migration. • Pigmented demarcation lines.
VKH Disease Clinical Course Chronic Recurrent Phase: • Acute episodes of granulomatous anterior uveitis with development of iris nodules • Recurrent posterior uveitis is distinctly uncommon • Complications are seen in this phase
VKH Disease Clinical Course Chronic Recurrent Phase: • Patients with recurrent VKH disease had a more intensive inflammation in the anterior segment and long-lasting dysfunction of the blood-aqueous barrier than those with initial onset VKH disease. Fang et al: Br J Ophthalmol 2008;92:182
VKH Disease Laboratory Investigations Diagnosis is made by clinical examination and ancillary test findings • Fluorescein angiography • Indocyanine green angiography • Ultrasonography • Optical coherence tomography • Multifocal electroretinograms • Lumbar puncture
VKH Disease Laboratory Investigations Ultrasonography: • Diffuse low to medium thickening of choroid. • Overlying exudative RD.
VKH Disease Laboratory Investigations OCT Useful in monitoring resolution of exudative retinal detachment On presentation 4 weeks after systemic corticosteroid
VKH Disease Laboratory Investigations Multifocal Electroretinogram • May be useful in detecting early retinal damage. • Macular function is severely impaired in patients with active uveitis. • Treatment with immunosuppressive agents leads to delayed but limited recovery of macular function. • May be useful in guiding therapy. Chee et al: Graefe’s Arch Clin Exp Ophthalmol 2005; 243:785. Yang et al: Am J Ophthalmol 2008; 146:767.
VKH Disease Retinal functional changes measured by microperimetry after immunosuppressive therapy • Patients displayed a markedly decreased BCVA, fixation stability and mean retinal sensitivity at baseline. • BCVA and fixation stability recovered earlier, faster and better than mean retinal sensitivity. • At final follow-up, retinal sensitivity was significantly reduced even in eyes with full recovery of BCVA. • Subclinical macular dysfunction is a permanent damage in VKH disease. Abu El-Asrar et al: Eur J Ophthalmol 2012; 22:368
VKH Disease Retinal functional changes measured by microperimetry after immunosuppressive therapy
VKH Disease Laboratory Investigations Lumbar Puncture: • Rarely necessary in a typical case. • CSF pleocytosis (mostly lymphocytes). • Transient and resolves within 8 weeks.
VKH Disease Laboratory Investigations Lumbar Puncture: • Frequency of CSF pleocytosis and the number of cells in CSF at disease onset were significantly higher in patients who eventually developed sunset glow fundus. Keino et al: Am J Ophthalmol 2006; 141:1140.
VKH Disease Complications • Cataract • Secondary glaucoma • Choroidal neovascular membranes • Subretinal fibrosis • Severe chorioretinal atrophy • Significantly associated with longer duration of disease and greater numbers of recurrences. Read et al : Am J Ophthalmol 2001;131:599. Sonoda et al: Jpn J Ophthalmol 1999;43:113.
VKH Disease Complications • Significantly associated with older age and more severe disease at presentation. Al-Kharashi, Abu El-Asrar: IntOphthalmol 2007;27:201
VKH Disease Therapy • Should be prompt and aggressive. • Systemic corticosteroids are mainstay of therapy. • 1-1.5 mg/kg/day of oral Prednisone (single morning-after-breakfast dose). • For 6-12 months with slow gradual tapering during this time. • Hospitalization with careful follow-up.
VKH Disease Therapy • Intravenous high-dose pulse steroid therapy (1g/day of Methylprednisolone given for 3 days) followed by oral Prednisone (1 mg/kg/day). • Topical Prednisone 1% solution and cycloplegics for anterior uveitis. • Patients adequately treated with corticosteroids have a fair visual prognosis. • Recurrences are associated with rapid or early decrease in steroid doses.
VKH Disease Therapy • Such treatment may shorten duration of disease, prevent progression into chronic stage, reduce incidence of extraocular manifestations. • Failure to prescribe proper corticosteroid therapy in initial phase may lead to chronic recurrent uveitis that may result in severe visual loss due to extensive chorioretinal atrophy. Sonoda et al: Jpn J Ophthalmol 1999;43:113.
VKH Disease Therapy • Final VA of 20/20 was significantly associated with use of systemic corticosteroids for longer than 9 months and slow tapering. • Recurrent inflammation was significantly associated with rapid tapering of systemic corticosteroids. Al-Kharashi, Abu El-Asrar: IntOphthalmol 2007;27:201
VKH Disease Therapy • Patients treated initially with immunomodulatory drugs (mycophenolate mofetil, cyclosporine A, azathioprine, and methotrexate) combined with corticosteroids had a better visual outcome than those who received corticosteroids as monotherapy. • Immunomodulatory therapy combined with corticosteroids should be considered as first-line therapy for patients with VKH. Paredes et al: OculImmunolInflamm 2006;14:87 Kim and Yu: OculImmunolInflamm 2007;15:381 Abu El-Asrar, et al: ActaOphthalmol 2012;90:e603
VKH Disease The outcomes of mycophenolate mofetil combined with systemic corticosteroids in acute uveitis associated with VKH disease • Use of mycophenolate mofetil as first-line therapy combined with systemic corticosteroids is safe and effective in the treatment of acute uveitis associated with VKH disease. • It has marked corticosteroid-sparing effect and significantly reduced development of chronic recurrent inflammation and late complications and significantly improved visual outcome. Abu El-Asrar et al: ActaOphthalmol 2012; 90:e603
VKH Disease Prognosis • Visual prognosis is generally favorable. • 87.5% achieved V.A. of ≥20/40. • High-dose systemic corticosteroids for >9 months with slow tapering significantly improves the prognosis and decreases risk of recurrence. • Age older than 18 years is significantly associated with the development of complications. • Visual prognosis is generally favorable in children. Al-Kharashi, Abu El-Asrar: IntOphthalmol 2007;27:201 Abu El-Asrar et al: Eye 2008;22:1124
VKH Disease Prognostic factors for clinical outcomes in patients treated with high-dose corticosteroids • Poor visual acuity and severe anterior segment inflammation at presentation are significantly associated with a worse outcome. • Chronic recurrent disease is significantly associated with more severe anterior segment inflammation and less exudative retinal detachment at presentation, more ocular complications and a worse visual outcome compared with initial-onset disease. • Use of immunomodulatory therapy as first-line therapy combined with systemic corticosteroids significantly improved clinical outcomes. Abu El-Asrar et al: ActaOphthalmol. In press.
Sympathetic Ophthalmia Ahmed M. Abu El-Asrar, MD, PhD
Sympathetic Ophthalmia • Rare bilateral granulomatous panuveitis that occurs as a complication of a penetrating injury that involves the uvea of one eye. • Accidental trauma or surgery. • Injured eye is referred to as the exciting eye and fellow eye as the sympathizing eye.
Sympathetic Ophthalmia Incidence • In 0.1% to 0.3% of patients after accidental trauma. • In 0.015% of patients following ocular surgery. • 5.8% and 0.67% after noncontact and contact Nd:YAG cyclotherapy, respectively. Allen: JAMA 1969;209:1090 Liddy, Stuart: Can J Ophthalmol 1972;7:157 Gass: Am J Ophthalmol 1982;93:552 Lam et al: Ophthalmology 1992;99:1818
Sympathetic Ophthalmia Incidence Role of ocular surgery • Sole cause in: • 45% of cases (Gass: Am J Ophthalmol 1982;93:552) • 17% of cases(Hakin et al: Eye 1992;6:453) • 28% of cases(Chan et al: Arch Ophthalmol 1995;113:597) • 56% of cases(Kilmartin et al: Br J Ophthalmol 2000;84:259) • 70% of cases (Su and Chee: Graefes’ Arch Clin Exp Ophthalmol 2006;244:243) • 38% of cases(Galor et al: Am J Ophthalmol 2009;148:704)
Sympathetic Ophthalmia Incidence Role of ocular surgery • Ocular surgery, particularly retinal surgery, is now a greater risk than accidental trauma. • Risk of one in 1152 retinal surgical procedures. Kilmartin et al: Br J Ophthalmol 2000;84:259 Su and Chee: Graefe’s Arch Clin Exp Ophthalmol 2006;244:243 Kilmartin et al: Br J Ophthalmol 2000;84:448