Download
1 / 1
10 likes | 122 Views
Patient Demographics, Complications, Hospital Utilization, and Accessibility of Care in 250 Consecutive Device Implants of a New Community Hospital Electrophysiology Program. Jeffrey L. Williams, MD MS FACC, David Lugg, Robert Gray, Douglas Hollis, Michelle Stoner, Robert Stevenson, MD.

E N D
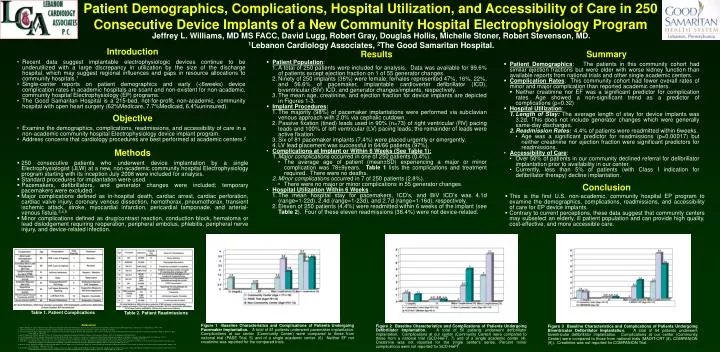
Patient Demographics, Complications, Hospital Utilization, and Accessibility of Care in 250 Consecutive Device Implants of a New Community Hospital Electrophysiology Program Jeffrey L. Williams, MD MS FACC, David Lugg, Robert Gray, Douglas Hollis, Michelle Stoner, Robert Stevenson, MD. 1Lebanon Cardiology Associates, 2The Good Samaritan Hospital. Introduction Results Summary • Recent data suggest implantable electrophysiologic devices continue to be underutilized with a large discrepancy in utilization by the size of the discharge hospital, which may suggest regional influences and gaps in resource allocations to community hospitals.1 • Single-center reports on patient demographics and early (<6weeks) device complication rates in academic hospitals are scant and non-existent for non-academic, community hospital Electrophysiology (EP) programs. • The Good Samaritan Hospital is a 215-bed, not-for-profit, non-academic, community hospital with open heart surgery (62%Medicare, 7.7%Medicaid, 6.4%uninsured). • Patient Population: • A total of 250 patients were included for analysis. Data was available for 99.6% of patients except ejection fraction on 1 of 55 generator changes. • Ninety of 250 implants (36%) were female; females represented 47%, 16%, 22%, and 56.6% of pacemaker, implantable cardioverter defibrillator (ICD), biventricular (BiV) ICD, and generator changes/implants, respectively. • The mean age, creatinine, and ejection fraction for device implants are depicted in Figures 1-3. • Implant Procedures: • The majority (98%) of pacemaker implantations were performed via subclavian venous approach with 2.0% via cephalic cutdown. • Passive fixation (tined) leads used in 90% (n=73) of right ventricular (RV) pacing leads and 100% of left ventricular (LV) pacing leads; the remainder of leads were active fixation. • Six of 81 pacemaker implants (7.4%) were placed urgently or emergently. • LV lead placement was successful in 64/66 patients (97%). • Complications at Implant or Within 6 Weeks (See Table 1): • Major complications occurred in one of 250 patients (0.4%). • The average age of patient (mean±SD) experiencing a major or minor complication was 78±9years. Table 1 lists the complications and treatment required. There were no deaths. • Minor complications occurred in 7 of 250 patients (2.8%). • There were no major or minor complications in 55 generator changes. • Hospital Utilization Within 6 Weeks : • The mean hospital stay for pacemakers, ICD’s, and BiV ICD’s was 4.1d (range=1-22d), 2.4d (range=1-23d), and 2.7d (range=1-16d), respectively. • Eleven of 250 patients (4.4%) were readmitted within 6 weeks of the implant (see Table 2). Four of these eleven readmissions (36.4%) were not device-related. • Patient Demographics: The patients in this community cohort had similar ejection fractions but were older with worse kidney function than available reports from national trials and other single academic centers. • Complication Rates: This community cohort had fewer overall rates of minor and major complication than reported academic centers. • Neither creatinine nor EF was a significant predictor for complication rates. Age showed a non-significant trend as a predictor of complications (p=0.32) • Hospital Utilization: • Length of Stay: The average length of stay for device implants was 3.2d. This does not include generator changes which were generally same-day discharges. • Readmission Rates: 4.4% of patients were readmitted within 6weeks. • Age was a significant predictor for readmissions (p=0.00017) but neither creatinine nor ejection fraction were significant predictors for readmissions. • Accessibility of Care: • Over 50% of patients in our community declined referral for defibrillator implantation prior to availability in our center. • Currently, less than 5% of patients (with Class I indication for defibrillator therapy) decline implantation. Objective • Examine the demographics, complications, readmissions, and accessibility of care in a non-academic community hospital Electrophysiology device implant program. • Address concerns that cardiology procedures are best performed at academic centers.2 Methods • 250 consecutive patients who underwent device implantation by a single Electrophysiologist (JLW) at a new, non-academic community hospital Electrophysiology program starting with its inception July 2008 were included for analysis. • Standard procedures for implantation were used. • Pacemakers, defibrillators, and generator changes were included; temporary pacemakers were excluded. • Major complications defined as in-hospital death, cardiac arrest, cardiac perforation, cardiac valve injury, coronary venous dissection, hemothorax, pneumothorax, transient ischemic attack, stroke, myocardial infarction, pericardial tamponade, and arterial-venous fistula.3,4,5 • Minor complications defined as drug/contrast reaction, conduction block, hematoma or lead dislodgement requiring reoperation, peripheral embolus, phlebitis, peripheral nerve injury, and device-related infection. Conclusion • This is the first U.S. non-academic, community hospital EP program to examine the demographics, complications, readmissions, and accessibility of care for EP device implants. • Contrary to current perceptions, these data suggest that community centers may subselect an elderly, ill patient population and can provide high quality, cost-effective, and more accessible care. Table 1. Patient Complications Table 2. Patient Readmissions References Figure 1 Baseline Characteristics and Complications of Patients Undergoing Pacemaker Implantation. A total of 81 patients underwent pacemaker implantation. Complications at our center (Community Center) were compared to those from national trial (PASE Trial, 5) and of a single academic center. (6) Neither EF nor creatinine was reported for the compared trials. Figure 2 Baseline Characteristics and Complications of Patients Undergoing Defibrillator Implantation. A total of 50 patients underwent defibrillator implantation. Complications at our center (Community Center) were compared to those from a national trial (SCD-HeFT, 7) and of a single academic center (4). Creatinine was not reported for the single center’s series. Percent minor complications were not reported for SCD-HeFT. • 1. Saba S, Ravipati, LP, Voigt A, “Recent Trends in Utilization of Implantable Cardioverter-Defibrillators in Survivors of Cardiac Arrest in the United States,” Pacing and Clinical Electrophysiology, Volume 32, No. 11 (Aug 2009), pp. 1444 – 1449. • 2. Grines CL and Keeley EC, “The Case for Emergency Transfer for Primary Percutaneous Coronary Intervention,” Circulation, November 29, 2005, pp. 3520-3532. • 3. Curtis JP, Luebbert JJ, Wang Y, Rathore SS, Chen J, Heidenreich PA, Hammill SC, Lampert RI, Krumholz HM, “Association of Physician Certification and Outcomes Among Patients Receiving an Implantable Cardioverter-Defibrillator,” JAMA, V. 301, No. 16 (April 22/29, 2009), pp. 1661-1670. • 4. Alter P, Waldhans S, Plachta E, Moosdorf R, Grimm W, “Complications of Implantable Cardioverter Defibrillator Therapy in 440 Consecutive Patients,” PACE, V. 28 (September 2005), pp. 926-932. • 5. Link MS, Estes NAM, Griffin JJ, Wang PJ, Maloney JD, Kirchhoffer JB, Mitchell GF, Orav J, Goldman L, Lamas GA, “Complications of Dual Chamber Pacemaker Implantation in the Elderly,” J Intervent Cardiac Electrophys, V. 2 (1998), pp. 175-179. • 6. Aggarwal RK, Connelly DT, Ray SG, Ball J, Charles RG, “Early complications of permanent pacemaker implantation: no difference between dual and single chamber systems,” Br Heart J, V. 73 (1995), pp.571-575. • 7. Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, McNulty SE, Clapp-Channing N, Davidson-Ray LD, Fraulo ES, Fishbein DP, Luceri RM, Ip JH, for the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators, “Amiodarone or an Implantable Cardioverter–Defibrillator for Congestive Heart Failure,” NEJM, V. 352, No. 3 (January 20, 2005), pp. 225-237. • 8. Moss AJ, Jackson Hall W, Cannom DS, Klein H, Brown MW, Daubert JP, Estes NAM, Foster E, Greenberg H, Higgins SL, Pfeffer MA, Solomon SD, Wilber D, Zareba W, “Cardiac-Resynchronization Therapy for the Prevention of Heart-Failure Events,” NEJM, V. 361, No. 14 (October 1, 2009), pp. 1329-1338. • 9. Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass DA, De Marco T, Carson P, DiCarlo L, DeMets D, White BG, DeVries DW, Feldman AM, “Cardiac-Resynchronization Therapy with or without an Implantable Defibrillator in Advanced Chronic Heart Failure for the Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure (COMPANION) Investigators, NEJM, V. 350, No. 21 (May 20, 2004), pp. 2140-2150. Figure 3 Baseline Characteristics and Complications of Patients Undergoing Biventricular Defibrillator Implantation. A total of 64 patients underwent biventricular defibrillator implantation. Complications at our center (Community Center) were compared to those from national trials (MADIT-CRT (8), COMPANION (9)). Creatinine was not reported for COMPANION Trial.






