Download
1 / 25
310 likes | 727 Views
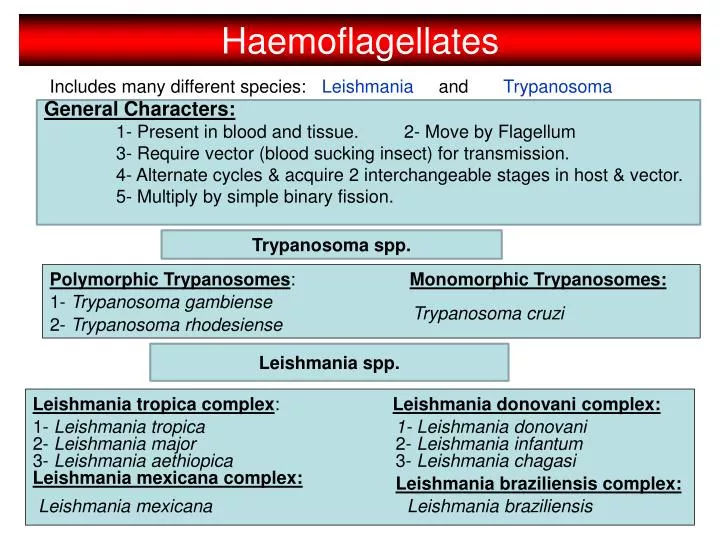
Haemoflagellates. Includes many different species:. Leishmania. and. Trypanosoma. General Characters: 1- Present in blood and tissue. 2- Move by Flagellum 3- Require vector (blood sucking insect) for transmission. 4- Alternate cycles & acquire 2 interchangeable stages in host & vector.

E N D
Haemoflagellates Includes many different species: Leishmania and Trypanosoma General Characters: 1- Present in blood and tissue. 2- Move by Flagellum 3- Require vector (blood sucking insect) for transmission. 4- Alternate cycles & acquire 2 interchangeable stages in host & vector. 5- Multiply by simple binary fission. Trypanosoma spp. Polymorphic Trypanosomes: Monomorphic Trypanosomes: 1- Trypanosoma gambiense Trypanosoma cruzi 2- Trypanosoma rhodesiense Leishmania spp. Leishmania tropica complex: Leishmania donovani complex: 1- Leishmania tropica 1- Leishmania donovani 2- Leishmania major 2- Leishmania infantum 3- Leishmania aethiopica 3- Leishmania chagasi Leishmania mexicana complex: Leishmania braziliensis complex: Leishmania mexicana Leishmania braziliensis
Blood Flagellates خيط flagellum (mastigote) then invade their tissues. 2- Transmitted to man through arthropods bite 1- Are Protozoa that swim in the blood of patients using & Trypanosoma Leishmania 3- Include: 4- Acquire the following shapes: Trypomastigote Amastigote Undulating membrane kinetoplast oval No free flagellum Free Flagellum Eccentric nucleus Central nucleus Promastigote Epimastigote kinetoplast Free Flagellum elongated kinetoplast Free Flagellum Central nucleus Undulating membrane Central nucleus
Leishmania spp. Introduction 1- Leishmania established everywhere in Forest, desert, mountains, towns, countries 2- Leishmaniasis is a variety of syndromes that are wide-spread giving rise to: Cutaneous – Mucocutaneous – Visceral Leisons. 3- Species variation & the cellular immune response determine the type of lesion 4- Leishmania spp. are strictly obligatory intracellular parasite of macrophages/ monocyte series (Histiocytes – Epitheloid cells – Kupfer cells – R.E.Cs 5- Multiply by binary fission within macrophages of : SKIN – RETICULO- ENDOTHELIAL SYSTEM & other VISCERA 6- Acquire interchangeable stages: Amastigotes: in Man- Dogs –Rodents. Promastigotes: in vector & culture 7- Transmission of the disease is seasonal – mainly zoonotic. Exceptionsare L. donovani in india & L. tropica ….. Whereas man is the only source of maintaining infection (Anthroponotic) 8- Vector of transmission is Sandfly “Phlebotomus” (old world) and “Lutzomyia” (new world).
Disease I- Cutaneous Leishmaniasis “Oriental Sore”: A- Old World Cutaneous Leishmaniasis (O.W.C.L.): 1- Single Dry Non-Exudative LesionL.tropica 2- Multiple Wet Exudative LesionL.major 3- Disseminated Cut. Leishmaniasis L.aethiopica 4- Chronic (Recidivan) Relapsing Cut. Leishmaniasis L.tropica B- New World Cutaneous Leishmaniasis (N.W.C.L.): 1- Relapsing skin Lesion (Chiclero’s Ulcer) L.mexicana 2- Mucocutaneous Leishmaniasis (Espundia) L.braziliensis II- Mucocutaneous Leishmaniasis “ESPUNDIA”: L. braziliensis III- Visceral Leishmaniasis “Kala-azar”: L. donovani - L. infantum - L. chagasi
Leishmaniacausesleishmaniasis Disease is caused by Bite of ♀ sandfly Liver Attacks human skin Old world cutaneousleishmaniasis Attacks human viscera New worldcutaneousleishmaniasis Old world visceral leishmaniasis Different Leishmania species New world visceral leishmaniasis
Mode of infection of Leishmaniasis Phlebotomus (OW) Lutzomyia (NW) Through the bite of female sand fly (vector) in skin or blood of patient block mouth & pharynx Amastigote Promastigotes Diagnostic stage Infective stage Alimentary canal of sand fly Promastigotes Multiply by binary fission Biological transmission
Transmission of Leishmaniasis _ by sand flies. _ artificial transmission of leishmania via the sharing of contaminated syringes and needles, from one intravenous drug user to another. Rarely, Leishmaniasis is spread from a pregnant woman to her baby (Materno-fetal transplacental transmission). Blood transfusion or contaminated needles also can spread Leishmaniasis.
Vector Female sand flies Male Female
Leishmania spp. Sand fly Amastigote Promastigotes of Leishmania
Pathogenesis & Clinical Picture of Cutaneous Leishmaniasis Nodule forms at the site of bite due to multiplication of Leishmaniain skin macrophages & granulomatous reaction around them. Inflammatory cells Promastigotes Amastigotes Skin macrophage forms with sharp-cut edges with raised indurated margin An ulcer In about 1 year Healing occurs leaving a disfiguring scar The patient develops solid immunity
Leishmaniaspecies causing ulcer in the Old World In the Middle East القرحةالشرقية 1- L. tropica 2- L. major Oriental sore المدن الريف Urban Rural dry chronic wet acute In Ethiopia & Kenya 3- L. aethiopica Affects patients producing diffuse cutaneous lesions resembling lepromatous leprosy. In patients withdeficientcell-mediated immunity Due to some characteristics of parasite species
I-Cutaneous Leishmaniasis “Oriental Sore”(O.W.C.L) 1- Single Dry Non-Exudative Lesion Caused by L. tropica URBAN type 1- Present in towns & cities (common in Saudi Arabia). 2- Long incubation Period (months to years). 3- Lesions develop in exposed parts such as (face –limbs) 4- Lesions are slowly progressive. 5- Ulcer heals “self-limiting infection” scar tissue form 6- C.M.I. curtails the infection leading to resistance to reinfection Appear as follows: single-small-Dry-painless nodule-nonexudative-delayed ulceration-small scar- non pruritic- uncommon 2ry bacterial infection. 2- Multiple Wet Exudative Lesion Caused by L. major RURAL type 1- Found in villages at edge of deserts(common in KSA). 2- Relatively short incubation period (2-6 weeks). 3- Lesions are more severe than L.tropica – big Ulcers 4- Lesions are rapidly progressive. 5- Dense nodules ulcerate & Coalesce big ulcers Appear as follows: Multiple-Big-Wet-painless nodule-Exudative 2ry bacterial delay healing –Big disfiguring scar- pruritic.
I-Cutaneous Leishmaniasis “Oriental Sore”(O.W.C.L) 3- Chronic (Recidivan) Relapsing Cut. Leishmaniasis Caused by L. tropica Few cases following primary skin lesion become hyper- Sensitive to parasite antigen --- vigorous immune response Persistent chronic infection (over years) The Lesions appear as follows:. 1- Papules develop around the healed skin & scar tissue 2- Ulcerate & heal by SCAR tissue formation 3- Appear as Tuberculoid skin lesion “Lupus Vulgaris”. N.B: Montengro’s Test (is strongly +ve), while smear & culture for parasite is –ve ???? 4- Diffuse Cut. Leishmaniasis (D.C.L.) L. aethiopica (also L. amazonensis) Inefficient cellular immune response limited cellular infiltration around infected macrophages failure of immune response to abort infection spread of amastigote The Lesions appear as follows:. 1- Multiple nodules with abundant parasite – Rarely ulcerate. 2- Skin becomes thick due to hyperplasia & hypertrophy. 3- The lesion appear as “Lepromatous Leprosy”.
I-Cutaneous Leishmaniasis “Oriental Sore”(O.W.C.L) somewhat like a volcano with a raised edge and central crater
Areas where Cutaneous Leishmaniasis exists L.tropica L.major In the Old World L.aethiopica L.infantum
Leishmaniaspecies causing ulcer in the New World L.peruviana L.braziliensis (Espundia) Dry ulcer (Uta) spread along lymphaticsto mucous membrane producing erosion of nasal septum, palate & larynx Leishmaniapifanoi Diffuselesion resembles lepromatous leprosy (does not heal or ulcerate).
Leishmaniaspecies causing ulcer in the New World Leishmania mexicana: single ulcer affects the ear causing destruction of the cartilage. (Chiclero’sulcer or Bay sore) L.braziliensis
I-Mucocutaneous Leishmaniasis “Espundia” Caused by L. braziliensis present in hot humid forest of central & south America 1- Vector of transmission is Lutzomyia. 2- majority of cases primarily present with Cutaneous Lesion 3- M.L. may develop 2-10 years following primary C.L.. 4- Deficient C.M.I. Spread of infection either directly or haematogenously to involve soft tissues of the Oronasal & Pharyngeal mucosa (NOSE-PHARYNX-LARYNX –UPPER LIP) 5-Lesion may be hypertrophy or severely destructive: Hypertrophy mainly NOSE & MOUTH. Destructive Mouth –Pharynx- Nasal (mucosa/cartilage Septum) nasal obstruction – bleeding – erosion massive destruction, severe pain & great deformity. N.B: only non-visceral Leishmaniasis lesion that may cause death from (Pneumonia- Septicemia as superimposed 2ry bacterial infection – malnutrition – Deficient C.M.I.)