Download
1 / 63
650 likes | 888 Views
Chronic Obstructive Pulmonary Disease (COPD). COPD is characterized by : **Chronic airflow obstruction & accelerated loss of lung function which is progressive & NOT fully reversible. ** COPD is preventable & treatable but NOT curable.

E N D
COPD is characterized by : **Chronic airflow obstruction & accelerated loss of lung function which is progressive & NOT fully reversible. ** COPD is preventable & treatable but NOT curable. **In COPD, airway obstruction is fixed & irreversible w/ different degrees of reversibility according to patients.
COPD is assoc. w/ abnormal response to noxious chemicals or gases. • Most common risk factor for COPD is SMOKING • COPD pts. experience: -productive cough -dyspnea **See table2 p.920 for comparative table b/w asthma & COPD
General Goals of Management of COPD: • Prevent or slow disease progression. • Relieve symptoms. • Improve exercise tolerance. • Improve overall health status. • Prevent & treat complications. • Prevent & treat exacerbations. • Decrease mortality.
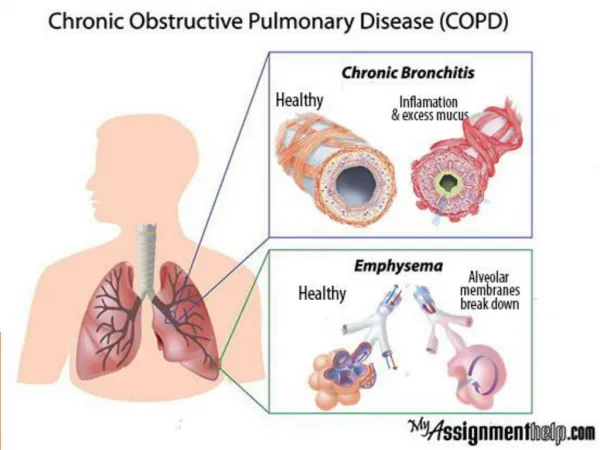
2 Major Forms of COPD: • Chronic Bronchitis (C.B.) • Emphysema 1) Chronic Bronchitis (C.B.): Defined clinically as chronic excessive secretion into bronchial tree occurring most days during a period of @ least 3 months /yr for @ least 2 consecutive yrs. 2) Emphysema: Defined anatomically as abnormal permanent enlargement of the alveoli distal to terminal bronchioles accompanied by destruction of their walls without fibrosis.
Both C.B.& emphysema are : • Indistinguishable. • Have different risk factors. • Have similar management strategies. ** Although Asthma & COPD are both characterized by airflow obstruction, their pathophysiologic features & response to treatment are different.
Etiology: *Smoking is major risk factor for COPD. • About 80-90% of COPD pts. have a history of current or past smoking although only 15-20% of smokers develop COPD due to genetic variation. • Other R.F. include: 1. Environmental factors(pollution&occupational) 2. Recurrent pulm. infections in childhood. 3. α₁ antitrypsin deficiency: Rare & inherited (<1% of emphysema cases)
Exacerbations of COPD typically have an infectious etiology, either viral or bacterial. • During an exacerbation, there is: • Increased S/S • Increased mucus production • Worsening of gas exchange • Worsening of airway obstruction assoc. w/ an increased risk of resp. failure.
Clinical Presentation & Diagnosis: • Clinical assessment of COPD pts. includes: 1) Medical history 2) Physical examination • Diagnosis of COPD is considered w/complaints of: *Chronic cough *Dyspnea *Sputum production * + History of risk factors
Signs & Symptoms: • Pathophysiologic changes progress over yrs. & clinical symptoms occur later. • By time pt. seeks med. help, disease is far advanced. • Sig. overlap b/w clinical presentation of C.B. & Emphysema. * Productive cough is assoc. more w/ C.B. • Dyspnea is more assoc. w/ Emphysema. • Obesity is assoc. w/ C.B. (Blue bloaters) • Wt. loss is assoc. w/ Emphysema (Pink puffers) • Gold standard for COPD diagnosis is spirometry: FEV1/FVC < 70% • When SABA is administered & spirometry is repeated in 15-30 min.: -COPD is typically characterized by < 12% improvement in FEV1 (or <200ml in pts w/ very low lung volumes). - A large increase in FEV1 is more consistent w/ asthma.
COPD progression may develop acute & chronic complications, i.e.: 1)Pulm. HTN 2)CorPulmonale & Rt. CHF ( Blue Bloaters ) 3)Polycythemia 4)Hypoxemia & resp. acidosis 5)Emphysematous (Pink Puffers)
An individualized approach to therapy should be: 1) Appropriate 2) Based on the severity classification 3) Patient’s risk factors • Important initial intervention: to reduce or eliminate exposure to risk factors. • Smoking cessation: the only treatment strategy proven to slow the chronic progressive loss of lung function.
Approaches to Treatment: • Pharmacotherapy: • None of the currently available therapies is shown to prevent or slow progressive loss of lung function. • 1⁰ role : symptomatic relief • 1⁰ strategy: using bronchodilators. • Response to meds. : Different among pts. • Assessment of response & S/Es (table35.8 p.926)
Reversibility of airflow limitation through spirometry (FEV1) : Not shown in many pts. • Dyspnea : Major debilitating symptoms for advanced dz. pts. • Inhaled route of adm.(MDI, DPI, Neb.): -Pref. because > effective, faster onset & safer than oral. -All inhaled mechanisms are equally effective in chronic management. -MDI & DPI: > convenient -Nebulizer: initial treatment in exacerbation.
*Bronchodilator combination used for additive benefits & reduced S/Es. 1) Bronchodilaters: A. Beta-2 Agonists: -SABA -LABA B. Anticholinergics: -SA Ach -LA Ach C. Methylxanthines
I. Bronchodilators: • Beta-2 Agonists: Examples of SABA: -Albuterol -Pirbterol -Terbutaline *Albuterol:- Most commonly used inhaled SABA. - < 5 min OA -Relativ. short DA ( ̴4hrs.w/chronic use) *In COPD, SABA: -Relieves symptoms -Improves exercise tolerance -No sig. lung function improvement
Examples of LABA: ( DA ̴12hrs) -Formoterol (OA ̴ 5min., pk. ̴ 30min.) Difference NOT -Salmeterol ( OA ̴ 15min., pk. ̴ 1-2 hrs.) important clinically *Sig. advantage of LABA over SABA *Considered for those NOT controlled w/ SABA • For more frequent or chronic symptoms, long acting bronchodilators (LABA, LA Ach.) are more effective in: 1. Improving lung function 2. Improving exercise tolerance 3. Improving quality of life 4. Reducing frequency of exacerbations
B) Anticholinergics: • Short Acting: Ipratropium Br.: (by inhalation) * ≥ bronchodilation than SABA @usual doses. *Little systemic absorption. *OA within 15 min., DA 4-6 hrs. *@ max. doses bronchodilation by beta-2 agonists maybe = to that of ipratropium in COPD but S/Es are more common w/SABA. *Due to slower OA, SABA may be preferred for acute bronchospasm w/ ipratropium used on scheduled basis. *Given as 2 inhalations QID increased to 6 inh. if needed.
2) Long Acting: Tiotropium: *Once daily dosing regimen. *Comparing Tiotropium w/Ipratropium in COPD: 1.Tiotrop. used QD, Ipratrop. used QID. 2. < Multiple exacerbations w/ Tiotrop. 3. Sig. longer time to 1st exacerbation w/Tiotrop. 4. For most outcomes, Tiotrop.> effective than Ipratrop. but > expensive.
Studies did NOT show significant clinical difference between LABA & Tiotropium in COPD management. • Short- acting bronchodilators (Albuterol + Ipratropium) combination increase effectiveness & as per treatment guidelines are commonly used in the management of Mild-Mod. COPD. • Limited data are available on the use of Long-Acting Bronchodilators combination, however, (LABA + Tiotropium) combinations are used for severe COPD patients.
C) Methylxanthines: • Theophylline is currently considered a 3rd- line agent in the management of COPD due to the availability of safer & more potent therapies & its risk of toxicities.
Issues to be considered with the use of Theoph.: 1) Different dosage forms &salts of theoph. are available.(SR QD or BID are most appropriate) 2) Significant variability in bioavail. between different products & patients. 3) Recommended therapeutic range for COPD 8-12ug/ml. 4) Smoking , other drugs, & disease factors interact w/ theoph. Careful monitoring of serum theoph. conc. is important. 5) Sig. S/E profile involves: GI, CNS, CV.
Summary of Bronchodilator Therapy: 1) Bronchodilators are the mainstay of therapy for chronic COPD management. 2) Inhaled form preferred over systemic. 3) Short-acting agents are used initially. 4) If symptoms continue, LA agents are >effective & convenient: Different trials showed long-acting bronchodilators (LABA & LA Ach) provided > benefit in improving different outcome measures than Short-Acting agents (SABA & SA Ach). 5) Bronchodilator combinations are commonly used with added benefit & reduced S/Es from higher doses of a single agent. 6) Oral theoph. Is an option reserved for those NOT responding to inhaled regimens or refuse to use inhaled meds.
II. Corticosteroids: • Did NOT result in dramatic response (unlike in asthma) which may be due to neutrophilic nature of COPD. • Systemic corticosteroid should be avoided in chronic COPD due to its lack of benefit & serious toxicity. • ICS has superior safety over systemic.
Current Guidelines suggest: Trial of ICS therapy warranted in patients: 1) whose FEV1 < 50%. & 2) who experience frequent exacerbations. *Newer ICS agents i.e.: -budesonide -fluticasone -mometasone May have less of a risk of S/Es.
Combination of LABA & ICS: -For convenience & ease of use. -Showed greatest FEV1 response w/ No difference in the exacerbation rate. *Mucolytic/Expectorant agents: - Showed NO clinical benefit in COPD. *Respiratory stimulants: -Not recommended due to short-lived effect + potential risk.
α₁-Antitrypsin Replacement Therapy: • Only used for the rare inherited form of emphysema. • Requires weekly or twice weekly infusions. • Not indicated for other forms of emphysema.
Non-pharmacologic Approaches: • Tobacco Cessation • Pulmonary Rehabilitation • Nutritional Therapy • Keeping Immunization Current • Supplemental O₂ Therapy
Tobacco Cessation: * Difficult to achieve & maintain. • The most important intervention in the prevention & treatment of COPD. • Slows the rate of loss of lung function • Most important & beneficial intervention • Associated w/ immediate & sustained health benefit.
2) Pulmonary Rehabilitation: • Patient Education ( ̴Dz., technique, adherence, self management skills). • Exercise Training. • Psychological Support & intervention (for anxiety & depression). d. Nutritional Therapy.
3) Nutritional therapy in COPD was shown to be valuable in: 1. Relieving symptoms 2. Improving exercise tolerance 3. Improving overall health status • Poor nutrition has sig. impact on COPD. • Pulm. Rehab.: • Less beneficial in preventing complications & exacerbations. • No effect in reducing mortality or slowing dz. progression.
4) Keeping Immunization Current: • The inactivated IM Influenza virus vaccine should be used because it has been shown to reduce serious illness & death in COPD pts. • Pneumococcal vaccine is recommended to be given SQ or IM because it provides prophylaxis against most common strains of Strep. Pneumiae.
5) Supplemental O₂ Therapy: (Long-Term Therapy) -Improves survival in COPD pts. w/ chronic hypoxemia. -Benefit seen if: - pO₂<55mmHg or -pO₂<60mmHg w/ evidence of end- organ effect of COPD, i.e.:*Corpulmonale *Polycythemia *Cognitive impairment
Greatest benefit shown in those who used O₂ for @ least 15hrs/d. • Nasal Cannula: The most common & convenient method of O₂ supplementation. • ABGs & Pulse Oximetry: The 1⁰ methods for determining O₂ saturation. • Goal of Therapy: Maintain O₂ saturation ≥ 90%. • Most are managed @ flow rates of 1-4L/min.
Surgical Management: • For those who can NOT be managed medically. • Bullectomy: -Removing bullea (large air spaces in lungs)not participating in gas exchange 2. Lung Volume Reduction Surgery (LVRS): -More common -More comprehensive procedure in removing non-functional segments of lung tissue. 3. Lung Transplantation:-Used in advanced COPD