Download

1 / 64
650 likes | 698 Views
The Picornaviridae family comprises small RNA viruses with non-segmented positive-strand RNA. Learn about their properties, classification, and medical importance, focusing on enteroviruses. Explore poliovirus characteristics, morphology, antigenic properties, and the mode of infection and pathogenesis.

E N D
PICORNAVIRIDAE FAMILY DR SATHYA ANANDAM
This family includes small RNA viruses containing single stranded non segmented positive strand RNA. IMPORTANT GENERAL PROPERTIES: • Small sized RNA viruses measuring about 20-30nm in size. 2) Icosahedral (cubical) symmetry. 3) Non enveloped viruses. 4) Molecular weight- 2.8 x 10.
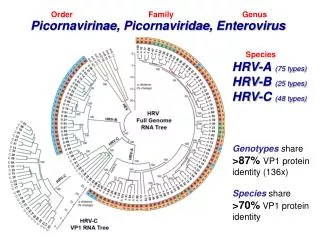
CLASSIFICATION The picarnoviridae family has been divided into 9 genera. However the following 6 genera have gained medical importance. 1) Genus Enterovirus (Enteroviruses) 2) Genus Rhinovirus (Rhinoviruses) 3) Genus Hepatovirus (Hepatitis A virus) 4) Genus Paraecho virus (Para ECHO viruses) 5) Genus Aphtho virus (Foot and mouth disease viruses) 6) Genus Cardiovirus (Cardioviruses)
ENTEROVIRUSES • The enteroviruses are relatively stable viruses surviving for long period in water, sewage, organic matter etc. • They resist pH of 3 for few hours. • Their calcium chloride density is 1.34gm/ml.
The enteroviruses of human i.e. Genus Enterovirus is subdivided into 5 species which include the following agents • Poliovirus- 1, 2, 3 types 2) Coxsackie viruses of group A- 1-24 types(except15,18 or 23) 3) Coxsackie viruses of group B- 1-6 types 4) ECHO viruses-1-34 (no types 10, 22, 23 and 28) 5) New enteroviruses- 68-78 except 72
POLIOMYELITIS POLIOVIRUS 1, 2, 3 types polios =“gray” myelos =“marrow” or “spinal cord” • Poliovirus is a typical Enterovirus which can survive in water, sewage, fecal matter for days to weeks. • The virus survives in milk, ice cream etc for long period. • It resist stomach acidity and routinely used chlorination of water (0.1ppm).
MORPHOLOGY • Virion: Spherical , 27–30 nm in diameter, contains 60 subunits • Composition: RNA (30%), protein (70%) • Genome: Single-stranded RNA, linear, positive-sense, infectious • Proteins: Four major polypeptides cleaved from a large precursor polyprotein. Surface capsid proteins VP1 and VP3 are major antibody-binding sites. VP4 is an internal protein. • Envelope: None • Replication: Cytoplasm
ANTIGENICPROPERTIES • 3 antigenic types : 1,2,3 • Prototype strain are : • Brunhilde & Mahoney : type 1 : Epidemics • Lansing & MEFI : type 2 : endemic • Leon & saukett : type 3 : epidemics. • By ELISA & CFT – 2 antigens can be recognized • They are • D [ dense] • C [ coreless or capsid]
HOST RANGE AND CULTIVATION: • Natural infection occur only in man • chimpanzees and monkeys can be infected experimentally • Primate cell culture like monkey kidney or human cell culture lines need to be used to grow virus in laboratory. • Infected cells round up, refractile and pyknotic, eosinophilic ontranuclear inclusion bodies
MODE OF INFECTION AND PATHOGENESIS • Source of infection- • Infected individual i.e. apparent or inapparent infection, convalescent carriers • The usual mode of infection is ingestion, rarely by inhalation. • The virus infects lymphatic tissue of GIT starting from tonsil topeyer’s patches of intestine and multiply.
After this primary multiplication the virus Spreads to regional lymph nodes and enters bloodstream(primary viremia) • Multiplies in RES---- secondary viremia • Through the blood virus reaches CNS & Spinal cord. The virus can also travel along axons of peripheral nerve to CNS(tonsillectomy). • The virus invades certain type of nerve cells-the anterior horn cells of spinal cord are more frequently and severely affected.
Reticular formation, vestibular nuclei, deep cerebellar nuclei and motor cortex of precentral gyrus are also involved. • The damage to neurons vary from mild chromatolysis to complete destruction of nerve cells with focal infiltration of lymphocytes, macrophages and plasma cells. • Occasionally lesions are seen in myocardium and peyer’s patches.
Pathogenesis:- Ingestion of contaminated water Reaches & multiplies in intestinal epithelial cells Further multiplication in peyer’s patches Enters to regional lymphatics Enters into blood stream (viraemia)
Seeded into CNS by blood Virus multiplies selectively in neurons Degeneration of Nissl’s bodies (chromatolysis) Aseptic meningitis In some cases progress to poliomyelitis
CLINICAL OUTCOME: • Incubation period - 7-14 days. • The poliovirus infection may follow one of the several courses: • 1) Asymptomatic/Inapparent infection (90%-95%) • 2) Abortive poliomyelitis (mild / minor illness) • 3) Non paralytic poliomyelitis (aseptic meningitis) • 4) Paralytic poliomyelitis • 5) Progressive poliomyelitis muscle atrophy
Abortive poliomyelitis • The minor illness is characterized by fever, malaise, headache, nausea, vomiting, constipation, sore throat, drowsiness- combination. • Recovery occur in few days.
NON PARALYTIC POLIOMYELITIS: • In addition to the signs and symptoms seen in minor illness stiffness and pain in neck and back, other signs of meningitis are present. • Recovery is noted in most of the cases in 2-10 days. • A small percentage of cases progress to paralytic disease.
PARALYTIC POLIOMYELITIS: • The classical presentation- flaccid paralysis, most often affecting lower limb as a result of damage to the lower motor neuron in the anterior horn of the spinal cord. • Respiratory paralysis may also occur due to involvement of brainstem. • If taken care, the possible maximum recovery may occur between 2-6 months ending ultimately with leaving behind varying degree of residual paralysis.
PROGRESSIVE POST POLIOMYELITIS MUSCLE ATROPHY: • Recrudescence of paralysis and muscle wasting has been observed in few individuals decades after paralytic poliomyelitis. • It does not appear to be a consequence of persistent infection, rather a result of physiologic and ageing changes.
LABORATORY DIAGNOSIS: • Virus recovery/ Isolation of virus- * In early cases from oropharynx (throat swab), * With the onset of clinical illness from rectal swab or fecal sample, * In fatal cases isolation can be done from brain, spinal cord or intestinal lymphatics
Human or monkey kindly cell cultures are inoculated, incubated & observed. • CPE appear in 3 – 6 days - Infected cells Round up & become refractile & pyknotic. • Isolated virus is identified and typed by neutralization with specific antiserum.
B) Serology- paired serum are required to show the antibody titer in course of the illness, a) CFT b) Neutralization test C) PCR of clinical specimen during early stage of disease THE VIRUS IS NOT DEMONSTRATED / RECOVERED USUALLY IN THE CSF.
IMMUNITY • Type specific • Passive immunity is from mother to off spring during the first 6 months of life. • Ig M , Ig G – Blood • Ig A, - Immunity against intestinal infection
PREVENTION AND CONTROL / PROPHYLACTIC MEASURES: • Nonspecific measures- a) Safe drinking water supply b) Improvement in sanitation c) Food hygiene 2) Vaccination- vaccine available a) Killed vaccine- SALK parenteral vaccine b) Live attenuated vaccine- SABIN oral vaccine
INACTIVATED POLIO VACCINE (SALK VACCINE) – 1953: • Killed parenteral vaccine • vaccine contains all the three types of polioviruses grown in monkey kidney cell lines and inactivated in formaldehyde. • Given by parenteral (IM) route.
The primary schedule includes 3 injections. • Adviced to begin when the baby is 2-3 months old • 2nd injection is after an interval of 6 weeks • 3rd injection is given after 6 months of second injection • First booster is given after 6 months and second booster is given around one and half year age of child.
LIVE ATTENUATED VACCINE (SABIN VACCINE)- 1959 • The routine use of this vaccine started from 1963. • Attenuated vaccine is prepared by serial passage of all the 3 types of poliovirus separately in cell cultures. • Each dose of this vaccine contains 1 lakh TCID50 of type 1, 2 lakhs TCID50 of type 2 and 3 lakhs TCID50 of type 3 poliovirus particles. • Stabilized using MgCl2 or Sucrose
SABIN VACCINE • The primary immunization consists of 3 doses (4 doses) starting at the age of 2 months. • The interval between 1st and 2nd dose is 4-6 weeks and interval between 2nd and 3rd dose is 6-8 weeks. • A booster when the baby attains the age of one and half year
THE ADVANTAGE OF LIVE ORAL POLIO VACCINE: 1) Easy to administer 2) Easy to convince the parent 3) The nature of immunity- both humoral and local 4) Duration of immunity is for longer period as vaccine virus stay in intestine and continuously stimulate the antibody production. 5) Use in epidemics is more practical. 6) Vaccine is cheaper than inactivated vaccine. However the virus has to be maintained / stored between 0-40C temperature continuously. This require an effective cold chain to ensure successful immunization.
VACCINE-ASSOCIATED PARALYTIC POLIOMYELITIS • affects approximately 1 person/2.6 million OPV doses distributed. • For immunocompetent patients, the clinical features and outcome of VAPP differ little from disease caused by naturally occurring polioviruses. • OPV virus types 3 and 2 are more common causes of VAPP than type 1.
Treatment : • Specific antiviral drugs for the treatment of poliomyelitis are not available, • management is supportive and directed to relief of symptoms
Eradication • Eradication is possible. • WHO has started the programme on 1988. • Aimed to eradicate the disease by 2000. • Poor progress in many countries a set back. • PULSE immunization : vaccine to all children in a region on a same day.
Global polio eradication initiative • To deliver sustained polio free world by • Detection and interruption of polio transmission • Immunisation strengthening • Withdrawal of OPV • Containment and certification • Legacy planning
INDIA : • 2006 – 60 cases were reported • 2011 till date only 1 case is reported West Bengal. Pulse polio immunization • OPV is given to children of 0-5 years age on single day, regardless to previous immunization • 2 rounds – 4-6 weeks apart • During low transmission season – nov - feb
A group of typical enteroviruses named after a place in NEWYORK state from where first member of this group was isolated in 1948 by DALLDROF & SICKLES. • There are 30 serotypes of coxsackie viruses which are divided into 2 groups as GROUP A & GROUP B • on the basis of their pathological lesions produced in injected suckling laboratory mice.
GROUP A COXSACKIE VIRUSES - 1-24 • Group A viruses cause widespread severe myositis of skeletal muscles resulting in generalized flaccid paralysis. • Signs of infection appear 4-5 days after the injection and the animal dies in next 4 or 5 days. • The coxsackie virus A23 now is placed in ECHO virus as ECHO virus 9.
GROUP B COXSACKIE VIRUSES – 1-6 The group B viruses produce widespread lesions in many organs • focal myositis, • necrosis of brown fat, • myocarditis, • Meningoencephalitis, • Pancreatitis and nephritis.
CULTIVATION OF COXSACKIE: • All the group B viruses grow well in monkey kidney cell cultures but only A7 and A9 grow in monkey kidney cells. • A21 can be grown on HeLa, HEp-2 or human embryonic kidney cell lines. • In cell cultures coxsackie viruses are cytopathogenic similar to polioviruses. • A7 and A14 can produce mild paralytic disease in monkey and adult mice.
CLINICAL CONDITIONS CAUSED BY COXSACKIE VIRUSES: Incubation period- 2-9 days. 1) Herpangina: vesicular pharyngitis Common coxsackie viruses responsible are A2 A3 A4 A5 A6 A8 A10. It is a self limiting severe febrile pharyngitis, sore throat with discrete vesicles on posterior half of palate, pharynx, tonsils and tongue. Usually seen in children.
2) Aseptic meningitis: Usual members responsible are B1-6, A7 and A9. Maculopapular rash may be present Self limiting illness. 3) Encephalitis: by B3. 4) Hand foot and mouth disease: Members usually responsible are A16, A9, rarely A4, A5, A7, A10. It is a self limiting illness characterized by oropharyngeal ulcerations, vesicular rash of palms and soles.
5) Myocarditis: Members responsible are B1-6, rarely A4 and A14. It is a serious disease seen in both children and adults. Infection is fatal in neonates or may cause permanent heart damage at any age. 6) Epidemic pleurodynia (BORNHOLM DISEASE): Caused by B1-6. Characterized by fever and stabbing chest pain of abrupt onset. Abdominal pain may be there. It is a self limiting disease lasting for few days to two weeks.
7) Diabetes mellitus: by B4 Abrupt onset of juvenile diabetes. 8) Generalized disease of infants: A extremely serious disease of early infants where multiple organs like heart, liver and brain are involved. Majority of cases progress rapidly with fatal ending. Few may recover completely. 9) Common cold like illness: by A10, A21, A24, B3. 10) Acute hemorrhagic conjunctivitis 11) Post viral fatigue syndrome
LAB DIAGNOSIS: • Recovery of the virus from throat wash, CSF, swab from lesions. 2) Isolation of virus by injecting to suckling mice or cell culture 3) PCR 4) Serology- neutralization test, immunoflorescence test, CFT.