Download
1 / 41
410 likes | 603 Views
Transfusion Reactions. Lloyd O. Cook, M.D. Department of Pathology March 2005. Definition: Txn Rxn. Any adverse outcome attributable to transfusion of a blood component or components. Immediate Action to Take for Txn Rxn: 1. STOP THE TRANSFUSION 2. Keep IV open with Normal Saline

E N D
Transfusion Reactions Lloyd O. Cook, M.D. Department of Pathology March 2005
Definition: Txn Rxn • Any adverse outcome attributable to transfusion of a blood component or components.
Immediate Action to Take for Txn Rxn: • 1. STOP THE TRANSFUSION • 2. Keep IV open with Normal Saline • 3. Check all blood component(s) labels, forms, Pt. ID for errors • 4. Notify Pt.’s physician as appropriate • 5. Treat rxn • 6. Notify Blood Bank; submit work-up specimens; submit report forms
Abnormal bleeding Chest/back pain Chills Coughing Cyanosis Dyspnea Facial flushing Fever (> 1 C ) Headache Hemoglobinuria Heat at infusion site Hypotension Itching Myalgia Nausea Oliguria/anuria Pulmonary edema Rales Rash Urticaria/hives Wheezing Uneasy feeling Common Signs & Symptoms
Selected Txn Rxns Signs/Symptoms Cause Management Prevention
Acute Hemolytic • Note: Most dangerous immunologic complication of Red Cell unit transfusion. • Usually due to clerical error: wrong Pt.; wrong blood component; etc. • High risk for morbidity or mortality. • Morbidity, e.g.: renal failure, DIC • Mortality: about 1 per 100,000 txn pts per year (cases reported to FDA)
Signs/symptoms (usual) Sudden chills Increased temp of 1 C to 2 C - fever Headache Flushing Anxiety Muscle pain Hemoglobinuria Low back apin Tachypnea Tachycardia Hypotension Vascular collapse Bleeding (N.B. surgical field in an anesthetized pt. Acute Renal Failure Hemoglobinemia DIC DIC with bleeding Shock Cardiac arrest DEATH Acute Hemolytic
Acute Hemolytic • Cause • Transfusion of incompatible donor RBC’s into Pt • Usually an ABO incompatibility • Antibodies in Pt plasma attach to antigens on donor RBC’s causing RBC destruction intravasculary • Antibodies fix complement causing RBC lysis
Acute Hemolytic • Management • Treat hypotension, renal failure, DIC, etc. • Submit blood samples for blood bank/laboratory tests • Avoid, if possible, further transfusions till work-up complete and/or Pt recovered from rxn
Acute Hemolytic • Prevention • Meticulously verify and document Pt ID from sample collection for compatibility testing through to blood component transfusion • Follow precisely the proper transfusion procedures at bedside (usually found in Nursing SOP’s ) every time – NO SHORTCUTS !!!
Febrile Rxn • Signs/Symptoms • Nonhemolytic • Sudden chills • 1 C to 2 C temp increase • Headache • Flushing • Anxiety • Muscle pain
Febrile Rxn • Cause • Pt immunologic sensitization to donor WBC’s, platelets or plasma proteins • Common sources: prior transfusions, previous pregnancies, previous transplants
Febrile Rxn • Management • Give antipyretics (e.g. aspirin – except children – Reyes Syndrome) • Avoid aspirin in thrombocytopenic pt’s • Do not restart transfusion
Febrile Rxn • Prevention • Consider leukocyte poor blood components • Two types of leukopoor RBC’s: filtered at time of donation and frozen/washed • Can also use WBC filters at bedside
Allergic Rxn • Signs & Symptoms • Flushing • Itching • Urticaria (aka hives) • Rarely, angioedema – epiglottal edema; bronchial airway constriction, hypotension, dyspnea, rales
Allergic Rxn • Cause • Pt sensitized to foreign plasma antigens • Exact mechanism not known for sensitization • Commonly caused by transfusion of plasma containing blood components, e.g.: FFP, Cryoprecipitate, Platelet Concentrates
Allergic Rxn • Management • Premedicate Pt with antihistamines (e.g. Benadryl) • If signs/symptoms mild &/or transient, restart transfusion after treatment • Do NOT restart transfusion if pulmonary symptoms/signs, fever present
Allergic Rxn • Prevention • Prophylactically treat with antihistamines
Anaphylactic Rxn • Signs & Symptoms • Note: very immediate type rxn • Anxiety • Urticaria • Wheezing • Severe dyspnea • Pulmonary/laryngeal edema • Shock • Cardiac arrest
Anaphylactic Rxn • Cause • Infusion of IgA proteins into Pt with IgA antibodies • IgA deficiency about 1 in 700 • Anaphylactic rxn rate about I per 1,000,000 pts. • Why disparity not known
TRALI • Transfusion Related Acute Lung Injury • aka Noncardiogenic pulmonary edema • Signs & Symptoms • Severe dyspnea • Hypotension • Fever • Chills • Bilateral pulmonary edema
TRALI • Cause • Donor antibodies activate Pt’s WBC’s which cause damage to blood vessels in lung tissue • Then fluids and proteins leak into alveolar space/interstitium • Mechanism similar to ARDS
TRALI • Management • Steroids • Aggressive ventilatory support • Hemodynamic support
TRALI • Prevention • Transfuse washed RBC’s from which plasma is removed • Platelet units can also be washed, but platelet function is significantly reduced
Circulatory Overload • Signs & Symptoms • Cough • Dyspnea • Pulmonary congestion • Headache • Hypertension • Tachycardia • Distended neck veins
Circulatory Overload • Cause • Iatrogenic – physician induced rxn • Fluid(s) administered faster than Pt circulation can accommodate volume load • Some at risk types of pt.’s: congestive heart failure, renal failure, hepatic cirrhosis, normovolemic anemia
Circulatory Overload • Management • Place Pt in upright position, if possible, with feet in dependent position • Diuretics • Oxygen • Morphine (if necessary)
Circulatory Overload • Prevention • Adjust transfusion flow rate based on Pt size and clinical status • Consider dividing unit(s) into smaller aliquot(s) to better space apart blood component(s) pace of transfusion
Septic Rxn • Signs & Symptoms • Rapid onset of chills & fever • Vomiting • Diarrhea • Profound hypotension • Shock
Septic Rxn • Cause • Transfusion of bacterially contaminated blood components • Common problem for platelet concentrates stored at room temperature
Septic Rxn • Management • Obtain blood cultures from Pt • Return blood component bag(s) to blood bank for further laboratory work-up • Treat septicemia with antibiotics • Treat shock with fluids & vasopressors
Septic Rxn • Prevention • Collect, process, store, transport, and transfuse blood components according to contemporary standards of practice (e.g. for FDA standards adhere to cGMP’s – current good manufacturing practices – found in Code of Federal Regulations) • Transfuse blood components within 1 to 2 hrs – do not exceed 4 hrs
Delayed Hemolytic Txn Rxn • Signs & Symptoms • Fatigue • Malaise • Declining hemoglobin/hematocrit • Conjugated bilirubin may be elevated • Falling hemoglobin/hematocrit usually noticed 3 to 14 days post transfusion
Delayed Hemolytic Txn Rxn • Cause • Anamnestic immune response in Pt to antigen(s) present on transfused donor cells • Antibody attaches to transfused RBC’s and RBC’s are removed from Pt’s circulation by reticuloendothelial system (liver/spleen) • This process is called extravascular hemolysis
Delayed Hemolytic Trn Rxn • Management • Send specimen(s) to Blood Bank for antibody identification work-up • Provide good Pt history
Delayed Hemolytic Trn Rxn • Prevention • Transfuse RBC’s that are phenotype negative for known clinically significant RBC antibodies in Pt • Delayed Hemolytic Trn Rxn’s can not be predicted • Good Pt records and Blood Bank records are essential • Clinical treatment usually not necessary
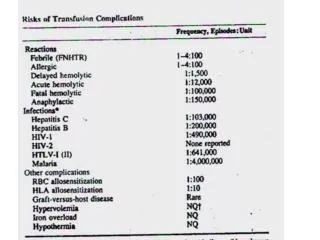
Txn Rxns Usual Incidence Rates • Some Selected Rates: • Acute Hemolytic ~1:32,000 • Febrile 1% to 2% • Allergic 1% to 3% • Anaphylactic ~1:170,000 to ~1:1,000,000 • Circulatory Overload ~1:10,000 • Delayed Hemolytic ~1:11,000
Infectious Risks of Transfusion(more common risk types) • Viral: • HIV 1 & 2 1:493,000 • HTLV-I/II 1:641,000 • Hepatitis B 1:63,000 • Hepatitis C 1:103,000
Infectious Risks (cont.) • Bacterial: • Red Blood Cells (RBC’s) 1:500,000 • Platelets, random 1:1:10,200 • Platelets, pheresis 1:19,000 • Parasites: • Chagas Dis. (T. cruzi) 1:42,000 • Malaria & Babesia <1:1,000,000
Txn Rxns - Reminders • Signs & Symptoms are usually nonspecific • No predictive tests for when a particular Txn Rxn will occur • Transfusion is an IRREVERSIBLE process – always benefits against risks • Be Prepared! – a Txn Rxn can happen unpredictably at anytime !!
Txn Rxns The End