Download
1 / 43
480 likes | 643 Views
Diplopia. Dr. Mohammed Alanazy. Versions - Terminology. Esotropia Exotropia Left Hypertropia. Diplopia.

E N D
Diplopia Dr. Mohammed Alanazy
Versions - Terminology Esotropia Exotropia Left Hypertropia
For horizontal diplopia, there are only four candidate muscles. Simply distinguishing an esotropia from an exotropia and determining the effect of lateral gaze identifies the weak muscle.
The two most common causes of horizontal diplopia are VI nerve palsy and INO • MG and thyroid eye disease must be considered in every case of diplopia if pupils are spared
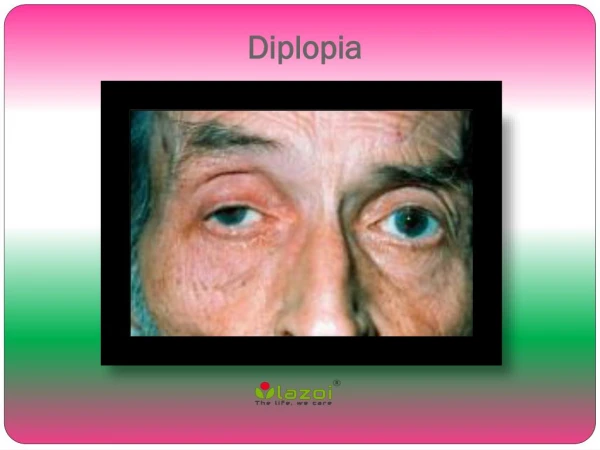
A 40-year-old man has vertical double vision that is worse in the evening. The patient has no other symptoms and denies head trauma or other systemic illness. Examination showed no apparent ocular motility disturbance.
1: Identifying the hypertropic eye. 2:Determining whether hypertropia increases in right-gaze or left-gaze IR (SO) SO SR(IO) SR
3:Determining whether the hypertropia increases with right head-tilt or left head-tilt. SO
Right 4th nerve palsy results in a right-left-right pattern. • Right hyperdeviation, worse in left gaze, worse on right head tilt. • Left 4th nerve palsy results in a left-right-left pattern. • Left hyperdeviation, worse in right gaze, worse on left head tilt.
Schematic of the third nerve nucleus and its fascicles in the midbrain. P, parasympathetic; IR, inferior rectus; IO, inferior oblique; LP, levator palpebra; CCN, caudal central nucleus; MR (a, b, c), medial rectus (three subnuclei); SR, superior rectus.
All patients with pupil-sparing partial palsies who do not undergo catheter angiography should be re-examined during the week following onset to ensure the pupil remains normal.