Download
1 / 72
740 likes | 1.29k Views
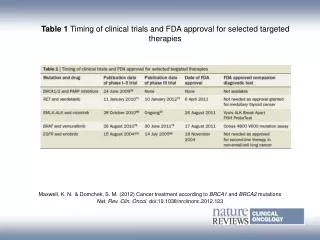
Lessons From Clinical Trials of Targeted Therapies for Cancer. George W. Sledge M.D. Indiana University Simon Cancer Cente r. What is Targeted Therapy?. Well-defined molecular target Target is correlated with tumor biology

E N D
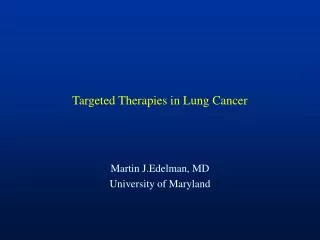
Lessons From Clinical Trials of Targeted Therapies for Cancer George W. Sledge M.D. Indiana University Simon Cancer Center
What is Targeted Therapy? • Well-defined molecular target • Target is correlated with tumor biology • Target is measurable in the clinic, or so common it doesn’t need to be • Target is correlated with therapeutic effect
The HER Family of Receptors TGF-α EGF Epiregulin Betacellulin HB-EGF Amphiregulin No ligand-binding activity* Ligands Heregulin (neuregulin-1) Epiregulin HB-EGF Neuregulins-3, -4 Heregulin Ligand- binding domain Tyrosine kinase domain Erb-B3 HER3 Erb-B1 HER1 EGFR Erb-B2 HER2 neu Erb-B4 HER4 *HER2 dimerizes with other members of the HER family. Roskoski. Biochem Biophys Res Commun. 2004;319:1. Rowinsky. Annu Rev Med. 2004;55:433.
Fluorescence In Situ Hybridization Test Measures HER2 Gene Amplification • FISH tests are designed to detect amplification of the HER2 gene Chromosome 17 centromere HER2 gene HER2-normalRatio <2.0 HER2-amplifiedRatio ≥2.0 PathVysion® PI. Revised May 2004.
Disease-Free Survival ACTH 87% 85% ACT 75% % 67% N Events ACT 1679 261 ACTH 1672 134 HR=0.48, 2P=3x10-12 B31/N9831 Years From Randomization
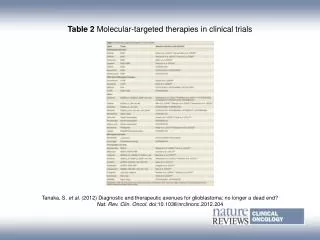
Targets for which Targeted Therapies exist • Steroid receptors: for ER+ breast cancer, prostate cancer, and lymphoma • HER2: for breast and gastric ca • ALK: for NSCLC • CD20: for lymphoma • bcr/Abl: for CML • c-Kit: for GIST • Hedgehog: for basal cell and medulloblastoma • RET: for medullary thyoid ca • b-RAF: for melanoma
Sort-of Targeted Therapy • VEGF-targeted therapies (except renal cell ca) • rarely drives tumor; hard to predict benefit • EGFR (colon, lung, H&N ca) • ras, EGFR mutations • CMF chemotherapy in high RS breast cancer • redefining targted therapy?
EGF Receptor: Role in CRC Therapy Meyerhardt & Mayer, N Engl J Med 2005 Venook, Oncologist 2005 pY PI3K pY pY pY PTEN STAT mTOR AKT Ligand Antibodies to EGFRcetuximab, panitumumab RAS RAF EGFR-TK MEK MAPK Gene transcription Cell-cycle progression Proliferation Survival (anti-apoptosis) Chemotherapy /radiotherapy resistance Invasion and metastasis Angiogenesis
Mutant – 7.4 vs 7.3 weeks Wild type – 12.3 vs. 7.3 weeks P= <0.0001
Oncotype DX 21 Gene Recurrence Score (RS) Assay 16 Cancer and 5 Reference Genes From 3 Studies PROLIFERATION Ki-67 STK15 Survivin Cyclin B1 MYBL2 ESTROGEN ER PR Bcl2 SCUBE2 GSTM1 BAG1 INVASION Stromolysin 3 Cathepsin L2 CD68 REFERENCE Beta-actin GAPDH RPLPO GUS TFRC HER2 GRB7 HER2
40 35 95% C.I. 30 Recurrence Rate 25 20 Rate of Distant Recurrence at 10 years 15 10 5 0 0 5 10 15 20 25 30 35 40 45 50 Recurrence Score Recurrence Score and Distant Recurrence-Free Survival Low RS < 18 Rec. Rate = 6.8% C.I. = 4.0% - 9.6% Intermediate RS 18 - 31 Rec. Rate = 14.3% C.I. = 8.3% - 20.3% High RS 31 Rec. Rate = 30.5% C.I. = 23.6% - 37.4% Paik .S. et al. N Engl J Med 2004;351:2817-26
B-20: Absolute % Increase in DRFS at 10 Years • Benefit of Chemo Depends on RS n = 353 Low RS<18 n = 134 Int RS18-30 n = 164 High RS≥31 0 10% 20% 30% 40% % Increase in DRFS at 10 Yrs (mean ± SE)
Targeted Therapies Vary in Effectiveness • Based on degree of “pathway addiction” • Is there an ideal target? • Based on drug-related issues
The Ideal Target? • Driving mutation in a • “Dumb tumor” that is • Easily druggable • and the mutation is really common
Dumb Tumors vs. Smart Tumors • CML, MTC, GIST • Non-Small Cell Lung Cancer: • Responses to EGFR and ALK-targeted therapy seen predominantly in non-smokers • Bronchial epithelium of smokers are loaded with mutations (~1 mutation/cell/3 cigarettes) • Breast Cancer: ER-neg vs. ER-pos • BRCA and BRCA-ness of TNBC; large mutational load • ER-pos: less LOH, more well-differentiated
Clinical Trial Implications of Biomarker-Driven Therapy • Number needed to study vs. Number needed to treat: a source of tension • Laboratory implications that follow from this
A Simulation of a Phase III Trial: Assumptions: Two subgroups (A and B) A is sensitive to targeted therapy and will have a 25% improvement in median survival from 2227 mo. B is insensitive to targeted therapy Three scenarios: A representing 100, 50, and 25% of the study population.
Crizotinib: Rationale for Development of a c-MET inhibitor • c-MET is potentially one of the most frequently genetically altered receptor tyrosine kinases in human cancers • Activating mutations • Hereditary papillary RCC: 100%, sporadic papillary RCC (13%) • HNSCC: 10% • NSCLC (8%) and SCLC (13%) • Gene amplification • Gastric carcinoma: 5-10% • Colorectal carcinoma: 4% primary tumors, 20% liver metastases • Esophageal adenocarcinoma: 5-10% • Anaplastic Lymphoma Kinase (ALK) (2 target for crizotinib) • Anaplastic lymphoma is very sensitive to chemotherapy • ALK point mutations and gene amplification are implicated in neuroblastoma … a rare tumor • ALK translocations in inflammatory myofibroblastic tumors … a very rare tumor
Crizotinib: Kinase Inhibition Profile Upstate 102 kinase Cellular selectivity on 10 of 13 relevant hits Crizotinib (PF-02341066) 13 kinase “hits” <100X selective for c-MET • Selectivity findings • ALK and c-MET inhibition at clinically relevant dose levels • Low probability of pharmacologically relevant inhibition of any other kinase at clinically relevant dose levels *The cellular kinase activities were measured using ELISA capture method Pfizer Inc. Data on file
A8081001: Phase I Trial of Crizotinib Cohort 6 250 mg BID MTD/RP2D Cohort 5 300 mg BID MDZ sub-study Cohort 4 200 mg BID Cohort 3 200 mg QD Cohort 2 100 mg QD MDZ sub-study Cohort 1 MTD = Maximum tolerated dose; RP2D = Recommended phase 2 doseMDZ = Midazolam (in-vitro data indicated that PF-02341066 is a major substrate and inhibitor of CYP3A activity) 50 mg QD Kwak EL, et al. ESMO/ECCO 2009(Abstract G6 and oral presentation)
Most Common Treatment-related Adverse Events (≥10%): Dose Escalation Cohorts (N=37) DLTs 3 objective responses observed in this part of the Phase I trial Kwak EL, et al. ASCO 2009 (Abstract 3509 and oral presentation)
Evidence for EML4-ALK as a Lung Cancer Oncogene • Insertion of EML4-ALK into NIH 3T3 fibroblasts was tumorigenic when implanted subcutaneously into nude mice • Engineered the specific expression of EML4-ALK fusion gene in lung progenitor cells using a surfactant protein C gene promoter • 100% of EML4-ALK transgenic mice developed lung adenocarcinoma that were + for ALK by IHC. No other primary cancers were observed. • Following IV injection of EML4-ALK/3T3 • cells into nude mice, all developed lung • cancer. Ten animals were treated with an • ALK-specific TKI and 10 were observed:
Key CollaborationPfizer and Massachusetts General Hospital Kwak EL, et al. ESMO/ECCO 2009 (Abstract G6 and oral presentation) • Of the 3 objective responders, all had ALK translocations: • Inflammatory myofibroblastic sarcoma: NPM-ALK translocation • NSCLC (2): EML4-ALK translocation
Clinical and Demographic Features of Patients with ALK-positive NSCLC Y Bang et al: ASCO 2010
Tumor Responses to Crizotinib for Patients with ALK-positive NSCLC Objective RR = 57% (95% CI: 46-68%) DCR (CR+PR+SD): 87% (95% CI: 77-93%) 60 40 20 0 –20 –40 –60 –80 –100 Progressive disease Stable disease Confirmed partial response Confirmed complete response Maximum change in tumor size (%) –30% * Y Bang et al: ASCO 2010 *Partial response patients with 100% change have non-target disease present
77% of Patients with ALK-positive NSCLC Remain on Crizotinib Treatment Individual patients • Reasons for discontinuation • Related AEs 1 • Non-related AEs 1 • Unrelated death 2 • Other 2 • Progression 13 0 3 69 12 15 18 21 Treatment duration (months) N=82; red bars represent discontinued patients Y Bang et al: ASCO 2010
Median PFS Has Not been Reached 1.00 0.75 0.50 0.25 0.00 PFS probability at 6 months: 72% (95% CI: 61, 83%) Progression-free survival probability Median follow-up for PFS: 6.4 months (25–75% percentile: 3.5–10 months) 95% Hall–Wellner confidence bands 0 2.5 5.0 7.5 10.0 12.5 15.0 17.5 Progression-free survival (months) Y Bang et al: ASCO 2010
Current Crizotinib Clinical Trials PROFILE 1007 • Crizotinib 250 mg BID (n=159) • administered on a continuous • dosing schedule RANDOMIZE • Key entry criteria • Positive for ALK by central laboratory • 1 prior chemotherapy (platinum-based) • Pemetrexed 500 mg/m2or • docetaxel 75 mg/m2 (n=159) • infused on day 1 of a 21-day cycle N=318 PROFILE 1005 • Key entry criteria • Positive for ALK by central laboratory • Progressive disease in Arm B of study A8081007 • >1 prior chemotherapy • Crizotinib 250 mg BID (N=250) • administered on a continuous • dosing schedule N=250 PROFILE 1007: NCT00932893; PROFILE 1005: NCT00932451
Crizotinib: The Good News • Important unmet medical need • Straightforward, biology-based biomarker predicting response • High response rate in heavily pre-treated patients (i.e., low NNT) • Relatively non-toxic A triumph for targeted therapy
Crizotinib as an Example: The Bad News • 4-5% of Non Small Cell Lung Cancer, so… • 20-25 patients screened for every EML4-ALK+ patient • Not all patients are trial eligible • Not all patients give informed consent • Best guess: 50+ patients screened for every patient entered on trial • Screening = FISH, which requires trained lab tech, time, and supply money • Lab requires CLIA certification
A Thought Experiment:Imagine ALK in Esophageal Cancer • Esophageal cancer = 16,640 cases/year, with 14,500 deaths • Assume ALK-like rates of gene expression of 5% • .05 X 16,640 = 832 patients/year in the US • Only 3% of patients with cancer go onto clinical trials • .03 X 832 = 25 patients/year entering trial
Medullary Thyroid Cancer • Thyroid cancer: 2% of all cancers • MTC: 5% of all thyroid cancers • RET proto-oncogene mutations drive • all hereditary MTC and ~50% of sporadic • RTKi’s for RET exist
Vandetanib • Inhibits VEGFR1,2, and RET • A dud in lung cancer • ASCO 2010: Phase III trial of 331 MTC patients • 54% reduction in rate of progression, p = 0.0001 • ORR 45% vs. 13% • International trial required; accrued in 1 year • NB: the “biomarker” was the diagnosis of MTC
It Gets Worse Multiple kinases are activated Optimal cell kill requires inhibition of multiple kinases Stommel et al. SCIENCE VOL 318: 287,2007
It Gets Worse • Assume: Cancers have multiple drivers • Targeting multiple RTK’s increases benefit • So now imagine esophageal cancers with two drivers, requiring two different targeted therapies • What is the number needed to screen to perform a trial of a combination of 2 RTKi’s?
Number Needed to Study:A New Concept for Biomarker-Driven Clinical Research • NNS = ___________1________ (fraction with biomarker X assay specificity X fraction trial-eligible X fraction giving informed consent X) Example: HER2+ = 1/(0.25 X 0.9 X 0.5 X 0.5) = 17.8 patients screened/patient entered into trial
NNS Implications • Fraction with biomarker is fixed by biology • Maximize true positives (specificity) by optimized assay development • Minimize number of exclusion criteria • Make trial as user-friendly as possible for patients
Problems With Biomarker Studies • Poor study design • Lack of assay reproducibility • Specimen availability issues • Issues with quantity, quality & preservation • Variability in assay results • Underpowered studies/overly optimistic reporting due to multiple testing, subset analyses & cut point optimization McShane, LM et al. J Clin Oncol 23: 9067-72, 2005
Phase of Trial: Preclinical 0 I II III IV Discovery Clinical Practice Pharmacokinetic Pharmacodynamic Prognostic CLIA Predictive If Assay Used For Individual Patient Decision Making Pharmacogenomic Research Lab Clinical Lab Assay & Marker Space
Clinical Assay Development Pipeline Assess assay performance in context: reproducibility, sensitivity, specificity, etc. Assess feasibility of detection/assay technology and marker prevalence Final late stage development, assay qualification Test cut-points in new retrospective specimen set Marker/technology discovery Set preliminary cut-points Test biomarker in retrospective set of specimens Trial activation
NCI Clinical Assay Development Program Patient Characterization Center (PCC) Clinical Assay Development Network (CADN) Clinical Assay Development Center (CADC) CADP: overarching program to move assays from research to the clinic CADN: network of CLIA certified labs providing services, including assay optimization, assessment of analytical performance, clinical validity in context of clinical trials PCC: internal lab performing gene expression profiling and somatic mutation detection using semi-quantitative NextGen sequencing on newly diagnosed cancers CADC: internal lab, part of CADN, the assay development arm of PCC; develop “high risk” standardized assays that can be disseminated Specimen Retrieval System/caHUB
Failure Rates of Investigational Drugs in Clinical Trials 9 of 10 drugs entering Phase 1 clinical trials will fail Historical timing of drug development failures 10% discontinuation in Phase 1 50-60% discontinuation in Phase 2 20-35% discontinuation in Phase 3
Why “Targeted” Agents Fail • The drug isn’t a drug • The drug isn’t used correctly • The drug is used in the wrong disease • Too much is asked of the drug • The drug is too toxic
SU5416 • Potent, selective inhibitor of VEGFR2 • Preclinical activity in animal models • Additivity/synergy with chemotherapeutics
SU5416: not a drug, a rock • High lipophilicity (Log P= 4.4), an extremely low aqueous solubility (< 10 ng/ml at pH 2-13) and low solubility in common pharmaceutically acceptable organic solvents (i.e., ethanol, PEG 400, propylene glycol, etc.) • Rapid clearance (half-life < 1 hour) • Major metabolites are inactive
18FDG-PET of patient with GIST treated initially with SU5416 and later with imatinib mesylate. Pre- and post- treatment with SU5416 Pre- and post- treatment with imatinib Heymach et al, CCR, 2004