Download
1 / 51
530 likes | 821 Views
Optical Coherence Tomography and Investigation of Optic Neuropathies. Dina Mohammed Abdulmannan Umm Al- Qura University. Optic Neuropathies. Demyelinating Compressive Ischemic Toxic/Nutritional Traumatic Hereditary Inflammatory/Infectious. Optic Neuropathies and OCT.

E N D
Optical Coherence Tomography and Investigation of Optic Neuropathies Dina Mohammed Abdulmannan Umm Al-Qura University
Optic Neuropathies • Demyelinating • Compressive • Ischemic • Toxic/Nutritional • Traumatic • Hereditary • Inflammatory/Infectious
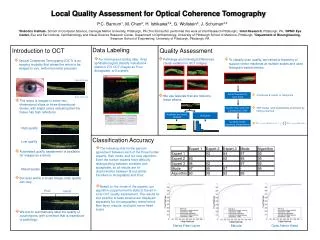
Optic Neuropathies and OCT • To monitor loss of retinal nerve fiber layer (RNFL) thickness • RNFL thickness is a reflection of axonal integrity in response to injury
Case 1: Anterior Ischemic Optic Neuropathy • 70-year old gentleman • “Blurred vision” in the right eye upon awakening • No Giant Cell Arteritis Symptoms • Vascular risk factors: Diabetes, Hypertension, and Dyslipidemia
Case 1: AION • Visual Acuity:20/40 OD 20/25 OS • Pupils:RAPD OD • IOP:19 mm Hg in both eyes • Fundus:Optic disc edema in the right eye. Absent physiological cup in the left eye
Case 1: AION Clinical Course • Vision worsened in the right eye after a week - Count fingers • No Symptoms of GCA • ESR = 6 mm per hour
OS OD Fundus Photos Optic disc edema (OD)
OS OD Case 1: AION and VF • MD -25.80 dB • Greater loss in superior field • MD -3.60 dB
Fast RNFL Thickness (3.4) 3.4 mm 1.92 seconds
Case 1: RNFL findings Mean RNFL = 52 µ • RNFL thinning in the right eye relative to the left eye • Greatest loss in inferior region correlating with superior VF loss Mean RNFL = 82 µ
Case 1: Anterior Ischemic Optic Neuropathy • OCT done 6 months following ischemic onset • What is timeline for axon loss to occur? • Does timeline differ across other optic neuropathies?
Case 2: Recurrent Optic Neuritis • 20-year old young woman • Developed “blurring” in the right eye • Pain with extraocular movements
Case 2: Recurrent Optic Neuritis Past Medical History • Bilateral optic neuritis in 1993 • treated with IV steroids • Cranial MRI scan normal • CSF analysis normal • No antecedent illness • Residual vision loss 20/40 OD and color vision deficit
Case 2: Recurrent Optic Neuritis • Recurrent optic neuritis in the right eye in 2000 • Repeat MRI scan normal • Vision recovered to baseline • Recurrence of optic neuritis in right eye in spring 2003
Case 2: Recurrent Optic Neuritis • Present Visual Acuity: 20/40 OD 20/20 OS • Pupils: Right RAPD • Fundus: Bilateral optic atrophy (temporal pallor)
OD OS Case 2: Visual Fields • MD -3.81 dB • MD -10.39 dB • Central loss greater in OD
OD OS RNFL Thickness • Bilateral RNFL thinning • worse in OD
Case 1: Recurrent Optic Neuritis • Few reserve axons remaining in OD • Following 3 bouts of optic neuritis • What extent of axonal loss will predict a permanent deficit in vision?
Case 3: Optic Neuritis • 32-year old woman • Diagnosed with MS in 1992 • Reported 6 recurrent bouts of optic neuritis affecting both eyes • Denied active optic neuritits at the time of examination
Case 3: Optic Neuritis • Visual Acuity: 20/25 OU • Pupils: left RAPD • Color Vision: 9/16 Ishihara plates in the right eye, and 6/16 plates in the left eye • Fundus: Bilateral optic atrophy
OD OS Case 3: Optic Neuritis MD -4.31 dB MD -3.03 dB
OS OD Case 3: Optic Neuritis • Residual central field depression OU • Greater in left eye
OD RNFL Thickness OS • RNFL thinning in the left eye relative to the right
RNFL vs Visual Field Loss • How well does the pattern of RNFL loss reflect or correlate with visual field loss in these patients?
Case 4: Compressive Optic Neuropathy • 18 year old male • Developed headache and vision loss in both eyes • Diagnosed with TB Meningitis • Large suprasellar tuberculoma • Causing compression of right ON and optic chiasm
Case 4: Compressive Optic Neuropathy • Visual Acuity: CF OD 20/25 OS • Pupils: Fixed pupil on right, with right RAPD (by reverse testing) • Ocular Motility: Right third nerve palsy with aberrant renervation • Fundi: Bilateral optic atrophy
OS OD Case 4: Compressive Optic Neuropathy • Dense central scotoma OD • Temporal cut OS
Case 4: Compressive Optic Neuropathy MRI: T1-weighted, post Gd Cystic Suprasellar Mass
Case 4: Compressive Optic Neuropathy Mean=40µ • profound bilateral RNFL thinning • worse in the right eye • OCT findings correlated well functional measures of visual integrity Mean=53µ
Case 5: Optic Neuritis? • 41-year old woman • Developed sudden onset vertigo and nausea in the fall of 2002 • Developed vision loss (nasal) and a floater and a “sparkle” in the right eye
Case 5: Optic Neuritis? • Visual acuity measured 20/20 in both eyes • Right RAPD • Color Vision 16/16 Ishihara plates in both eyes • Fundi: Examination normal
Case 5: Optic Neuritis? • The visual field defect persisted • Cranial MRI scan normal • Orbital CT scan normal • CSF analysis normal
Case 5: Optic Neuritis? OS OD • Mean Deviation – 0.31dB • Normal field • Mean Deviation -7.55 dB • Nasal superior and inferior visual field loss
Case 5: Multifocal ERGs mERG Trace Arrays Retinal view Retinal view OD OS • Multifocal ERG recordings from 61 regions in the central 45 degrees • mERG trace arrays appear reduced in inferior and superior temporal retina in OD • mERG trace arrays appear normal in OS
Case 5: Multifocal ERGs Statistical Probability Maps OD OS SPM 85 normal eyes The Patient • Statistical probability mapping of response density was normal in OS • Reduced response density in inferior and superior temporal retina in OD • Correlates with visual field defect in OD
RNFL • RNFL thickness within normal limits OU • Good RNFL symmetry between eyes
Case 5: Optic Neuritis? • In May, 2003 the patient reported new “sparkles” in the left eye Summary: • Atypical Optic Neuritis • MS work-up negative • Lack of optic disc pallor • Persistent visual field defect • Positive visual phenomena and floaters in both eyes
Case 5: Optic Neuritis? • Diagnosis: Acute Zonal Occult Outer Retinopathy
Case 5: Optic Neuritis? • The clinical distinction between a retinal versus an optic nerve problem may be difficult • Ancillary studies such as OCT and mERG can be very useful in this regard
Case 6: Traumatic Optic Neuropathy? • 61-year old woman was hit with a tennis ball in the left temple in October 2002 • Developed chronic headaches • Noted inferior visual field loss in the left eye • Referred to the Neuro-Ophthalmology Clinic in January 2003
Case 6: Traumatic Optic Neuropathy? • Visual Acuity: 20/20 in the right eye and 20/25 in the left eye • Pupils: Equal with no RAPD • Color Vision: 15/16 Ishihara Plates in the right eye, and 12/16 plates in the left eye • Fundi: Normal
Case 6: Traumatic Optic Neuropathy? • Serology Studies- Normal • Cranial/Orbital CT scan- Normal • Orbital Ultrasound- Normal
Case 6: Traumatic Optic Neuropathy? • In April, 2003 the patient developed new visual field loss in the right eye • In May, 2003 she noted sparkles, flashes, and floaters in both eyes
MD -6.91 dB MD -0.64 dB OD OS Case 6: Traumatic Optic Neuropathy • Visual Fields Obtained in March 2003 • OD-Normal • OS-defects in superior and inferior
MD -7.81 dB MD -2.41 dB OS OD Case 6: Traumatic Optic Neuropathy? • Visual Fields obtained in April 2003 • OD- now developing VF defects • OS- visual defects worsened
Case 6: Traumatic Optic Neuropathy? Repeat Examination • Visual acuity: 20/25 in both eyes • Pupils: equal with no RAPD • Color Vision: 12/16 Ishihara Plates in the right eye, and 7.5/16 plates in the left eye • Fundi: Normal
Case 6: Traumatic Optic Neuropathy? mERG Trace Arrays Retinal view Retinal view OD OS • Multifocal ERGs from 61 regions in the central 45 degrees • mERGs from OD are diminished centrally extending to superior nasal retina • mERGs from OS show multiple patchy areas of abnormality
Case 6: Traumatic Optic Neuropathy Statistical Probability Maps OD OS • Statistical probability mapping shows areas of significantly reduced response density centrally and in superior nasal retina in OD • OS shows much greater involvement in response density reduction in inferior and superior retina
RNFL • RNFL thickness within normal limits OU • Good RNFL symmetry between eyes
Case 6: Traumatic Optic Neuropathy? • Diagnosis: Acute Zonal Occult Outer Retinopathy • Para-neoplastic work-up was recommended by Retinal Specialist