Download
1 / 55
600 likes | 725 Views
Discover the crucial role of autocoids, including histamine and serotonin, in allergic reactions, inflammation, and various physiological functions. Learn about their classification, locations, mechanisms of action, toxicity, clinical uses, and interactions. Explore the pharmacological effects and clinical applications of histamine H1-receptor antagonists and second-generation antihistamines in treating various conditions.

E N D
AUTOCOIDS BY PROF. A. ALHAIDER Department of Medical Pharmacology College of Medicine
Definition: Auto = self Coids = Remedy or some times called Local Hormones Why are they very important?
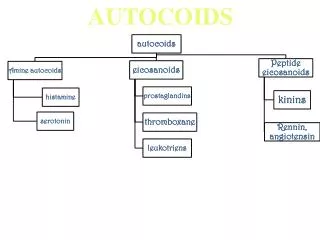
Classifications: A. Amine Autociods: 1. Histamine 2. Serotonin B. Eicosanoids (PGs; Thromboxane ; Leukotriens) C. Peptides Autociods: 1)Kinins 2) Renin; Angiotensins etc) 4. Endogenous peptides (Kinins; Renin; Angiotensins etc)
HISTAMINE • Locations: mediators of allergic and inflammatory reactions; also involved in Gastric Acid Secretions ; and as Neurotransmitter & Neuromodulator. • Thus, it is located in: a) Mast cells (lung,skin, GIT, BV…etc) b) Basophiles, Platelets, Enterochromaffin- like (ECL) cells of the stomach c) Brain
Storage and Release: • Histamine is usually found in storage granules as complex with sulfated polysacharides, heparin and released (locally) by: a) Immunologicl Mechanism (see Fig 56-5) b) Tissue injury Mast cell degranulation c) Chemical and physical Conditions ( see table 51-2)
Mechanism of Action: Histamine binds to three types of Receptors , namely H1 , H2 , H3 (see table 16-1) Which one of them localized presynaptically?.
Effects on Organs • a) CVS: systolic and diastolic blood pressure Heart rate. Heart Contracility b) GIT: Gastric acid secretion (H2) (very important) Contractility (but less in human) C)Bronchial smooth muscle contraction and secretion. What is the significant of such an effect? d) Nerve ending (Pain & Itching)
Toxicity and contraindications: • How does it occur? • Manifestations • Treatment
Histamine H1 – Receptor Antagonists Histamine can be antagonized by the followings: • a) Physiological Antagonism by epinephrine • b) Mast cell release inhibitors (Sodium Chromoglycate) • C) Histamine Receptors Antagonists (The Most Important Clin. Approach)
Pharmacokinetic of H1-antagonists) ( see Table 16-2) • They are divided into first & Second Generation based on t ½ and lipophilicity. • Drugs that inhibit (Cyto.P450), will increase the cardiac toxicity of the piperidines derivatives.
Pharmacodynamics: • Pham. Actions of H1 –antagonists could be attributed to their H1, Muscarenic, alpha- adrenergic or serotonergic actions • a) Antagonize Histamine Actions (e.g. Edema = capillary permeability; vascular response; effects on smooth muscle) • These effects are utilized clinically for Allergy? • b) Sedation (First Gen.) Is it useful? • c) Antinausea & Antiemetic Actions I( First Gen.) • d) Anticholinergic (first. Gen) Is it useful?. • e) Strong serotonin blockade (Cyproheptadine) • f)↓ Bronchial and nasal secretion • G) Local anesthetics
Clinical Uses: • a) Allergic Reactions (e.g.: Allergic Rhinitis ; Urticarea , etc. • b) Motion Sickness & Vestibular (Cyclizine; Meclizine) • c) Nausea & Vomiting of Pregnancy (Doxylamine (BendectinR) • Local anesthesia: first generation (Diphenhyramine and promethazine) Why Antihistamines are not used for Asthma?.
Side Effects: Should be predicted from the pharmacological effects? Plus drug allergy after local uses. • Receptors selectivity: 1st generation antihistamines are of poor H1 receptor selectivity. They block other receptors leading to adverse effects: • Cholinergic R blockade: dry mouth, urinary retention, & tachycardia • -adrenergic R blockade, by promethazine, leading to hypotension, tachycardia & dizziness • Serotonin R blockade leading to increased appetite (Cyproheptadine) • Drug Interactions: • Liver microsomal Enzyme inhibitors increase the arrythmogenic action of piperridine second Gen (Astemazole and Terfenadine). . Sedative actions of antihistamine increase if given with alcohol or any sedative drugs
Serotonin • Definition and Location: • it is a neurotransmitter found in enterochromaffin cells in GIT (90%) , and in plateletes and in raphe nuclei of brain stem. • Is serotonin as important as N.E or Histamine?
Mechanism of action : Interacts with 12 receptor subtypes (see Figure 16-4) • Why is 5-HT3 receptor differs from other 5- HT receptors?
Pharmacological actions of Serotonin • CVS: 1) Blood vessels: Potent and direct contractions on smooth muscle (via 5- HT2) EXCEPT : Skeletal Muscles and Heart blood vessels. • Note : 5- HT can give rise to triple action: Decrease BP due to chemoreceptor response then increase BP due to Vasoconstriction (5-HT2), then decrease B.P due to skeletal muscle V.D 2) Platelet: Increase platelet aggregation via 5-HT2
GIT: • 1) increase contraction of smooth muscle (via 5- HT4 stimulated the release of ACH). • What is the clinical significant? 2) Nausea and vomiting (via 5-HT3) therefore 5-HT3 antagonists are used for RX of ? • Respiration : 5-HT may produce weak bronchoconstriction. • CNS: very important.(Appetite; depression and mania; Pain; Anxiety; Schizophrenia).
Clinical Uses of Serotonergic Drugs: • Note1: Unlike NE or DA, serotonin its self has no clinical uses, however, it agonists and antagonists have very important therapeutic applications. • Note 2: Unlike histamine where only its antagonists are used, serotonin agonists and antagonists can be used.
Clin. Uses of Serotonergic Agonists: 1) Buspirone: 5-HT1A agonist used as anxiolytic agent. 2) Sumatriptan: 5-HT1D agonist for migraine (Treatment and prophylactic). 3) Metoclopromide (Plasil): 5-HT4 agonist as prokinetic agent (for Rx of gastroesophagial reflex). How does it work? And also used for N/V via 5-HT3 antagonistic action. 4) Dexfenfuramine: Acts by stim. Release and inhib. Reuptake of serotonin. Used as anorexic agent. What is the effect of serotonin antagonists on appetite?
Clinical Uses of Serotonergic Antagonists: 1) Ondansetron & Granisetron: 5-HT3 antagonists Common used for Rx of N/V induced by cytotoxic (chemotherapy) drugs. 2) Cyproheptadine: Both H1, 5-HT1,2 and cholinergic antagonist used for Rx carcinoid tumor (significant increases in serotonin) and to increase appetite.. 3) Ketanserin: 5-HT2/1c antagonist and a1-adrenergic blocker. (used as antihypertensive agent) 4) Methysergide: This is an ergot alkaloid acts as 5-HT1,2 antagonist used for Rx of migraine.
Ergot Alkaloids • Produced from fungus with a pharmacologically nonspecific actions at a-adrenoceptors, dopamine and 5-HT. • Basic Pharmacology • What is Ergot poisoning? • MOA: Act on several types of receptors either agonist, partial agonist, or antagonists (see Table 16-6) (simply act on a-adrenoceptors); Dopamine and 5-HT). • CNS: • Stimulation of 5-HT2receptors leads to hallucinogenic action (e.g.: by LSD) • Stimulation of dopaminergic receptors especially in the pituitary decrease prolactin release and emoliorate the symptoms of parkinsonism (e.g: Bromocriptine)
CVS: • Vasoconstriction via a-adrenoceptors and 5-HT2 receptors (Ergotamine via a1 and increase NE) Uterine Smooth Muscle: Why they are more effective in pregnancy? (e.g.: Ergonovine) Clinical Uses of Ergot Alkaloids • Migraine (Ergotamine (with caffeine) or dihydroergotamine during the attack while methysergide for prophylaxis) • Hyperprolactenemia (Bromocriptine= Dopamine Agonist)) • Parkinsonism (Bromocriptine = Dopamine Agonist) • Post partum hemorrhage (Ergonovine) To induce vasoconstriction. • Diagnosis of variant angina (Ergonovine) Toxicity: GIT as diarrhea; N/V; Prolongs vasospasm (ergotamine and ergonovine) may progress to gangrene.
Eicosanoids • Definition: • Classifications; (see figures 18-1; 18-2 ;18-3) • a ) Cyclooxygenase derivatives (prostaglandins and thromboxane) • b) Lipoxygenase products ( leukotriens)
Synthesis of eicosanoids and sites of inhibitory effects of anti-inflammatory drugs Membrane lipid Corticosteroids Arachidonic acid NSAIDs Hydroperoxides Endoperoxides (HPETES) (PGG, PGH) Leukotrienes Prostacyclin Thromoxane (LTB, LTC ,LTD, LTE) (PGI) (TXA) Prostaglandins (PGE, PGF) Phospholipase A2 - Cycloxygenase Lipoxygenase -
Physiological and Pharmacological Actions of Eicosanoids Mechanisms and Receptors: Act on cell surface receptors All coupled to G-protein. PGI; PGE increases adenylate cyclase (decrease intracellular calcium) while TXA2 increases IP3 (increases intracellular calcium) Pharmacological & Physiological Effects: (Table 1 & 13-1) A. Uterine Tone • Blood pressure regulation (Dilatation and constriction) • Inflammation • Gastric Secretion and motility. • Platelet aggregation • Bronchial tone • Effect on kidney H. CNS (Fever; Pain; Sleep) J. Eye
Table 1: Effects of some eicosanoids ↑= slight increase, ↑↑= moderate, ↑↑↑=high, ↑↑↑↑=very high, ↓= slight decrease, ↓↓= moderate and, ↓↓↓= marked; ?= unknown effects
Clinical Uses of Eicosanoids and Inhibitors: • A. Uses of Eicosanoids: • Oxytocis agents: (e.g.: Dinoprostone PGE2) vaginally or Misoprostol (p.o) • _ - Impotance: Alprostadil PGE2 • _ -Glaucoma: Latanoprost PGF2 • Pulmonary Hypertension ( PGI2 or prostacyclin, Epoprostenol) • Peptic Ulcer (PGE1 Misoprostol (Cytotec) • B – uses of eicosanoids blockers: • Asthma: Leukotrien antagonists (Zafirleukast; Montelukast); or Lipoxegenase inhibitor e.g. Zileuton • Anti-inflammatory and RA (NSAIDs) • Antiplatelet action (Aspirin) • Dysmenorrhea (NSAIDs)
C. Vasoactive Peptides • A. Vasoconstrictors (angiotensin II; vasopressin; endothelins and neuropeptide Y. • B. Vasodilators (Bradykinin and related Kinins; Natriuretic Pepties; Vasoactive Intestinal Peptide; substance P; Neurotensin)
Kinins : (e.g. : Bradykinin & kallidin) • Polypeptides present in plasma and several tissues including the kidneys, pancreas, intestine, sweat and salivary glands. ACTIONS : CVS: Very potent vasodilator (direct and via increase EDRF). Also, increases the body capillary permeability
Bronchioles : Contraction of bronchial smooth muscles (cough). • Inflammation : Kinins can produce all the symptoms of inflammation (pain and edema when injected to tissue). • Pain : Intradermal injection of kinins elicited potent pain (Stimulate nociceptive nerve afferent fibers) • DOES BRADYKININ PLAY ANY ROLE IN THE MECHANISM OF ACTION OF ACEIs?
Natriuretic peptides: Locations: Atrial (ANB) and Brain (BNP) (Found in ventricle as well) Clinical significant: (increase in heart failure; renal failure; SISADH Actions: decrease the secretion of renin, aldosterone and vasopressin; decrease blood pressure and increase sodium excretion. Act via activation of guanalyl cyclase. Calcitonin: from thyroid and the most potent vasodilators in the body. Vasoactive-intestinal peptides: Vasopressin (Antidiuretic hormone ADH) Uses: Supstnace P:is an arteriolar vasodilator that is also pain-mediating neurotransmitter but causes venoconstriction and bronchoconstriction. Capsaisin releases substance P from nerve ending (used for arthritic joints and for postherpetic neuralgia).
Include atrial natriuretic peptide (ANP), brain natriuretic peptide (BNP), C-type natriuretic peptide (CNP) ANP derived from a 126 amino acids prohormone, secreted primarily from cardiac atria BNP, identified initially in brain, is secreted from both atria & ventricles CNP identified in brain & in vascular endothelial cells Stretch receptors in the atria and ventricles detect changes in cardiac chamber volume related to increased cardiac filling pressures, resulting in release of both ANP and BNP but not CNP The Natriuretic Peptide Family
The Natriuretic Peptide Family • The actions of the natriuretic peptides are mediated by natriuretic peptide receptors (NPRs),NPR-A/B/C • NPR-A & NPR-B are coupled to membrane-bound GC, increases levels of cGMP • NPRs are localized in vascular SM, endothelium, platelets, the adrenal glomerulosa, & the kidney • ANP & BNP increase urine volume & sodium excretion, decrease vascular resistance, and inhibit release of renin and secretion of aldosterone & vasopressin • Neutral endopeptidases (NEPs) inactivate NPs