Download
1 / 16
160 likes | 223 Views
Learn about common vulvovaginal infections like Candidiasis and Bacterial Vaginosis, their symptoms, treatments, and preventive measures. Understand gerontologic considerations and nursing care. Explore reproductive health challenges in adolescents, including pregnancy risks and complications. Discover strategies for promoting maternal and infant well-being.

E N D
Vulvovaginal infections • Infections very common • Normal vaginal defenses: pH 3.5 – 4.5 • Maintained by normal flora: Lactobacillus acidophilus • Nsg goal: prevent re-occurrence of infections • Reduce stress and illness • Maintain normal pH • Avoid introduction of pathogen
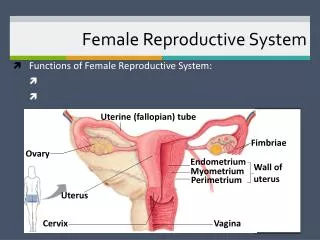
Vaginitis • Inflammation of the vagina • Causes: Candida or Trichomonas • Vaginal discharge • Urethritis may develop due to close proximity of the urethra • Sx. Redness, burning, ithing, odor, edema • Tx: oral or local medication
Candidiasis • Fungal or yeast infection – Candida albicans • May be present without symptoms • Common in pregnancy, DM and HIV • Also common I patients taking corticosteroids or oral contraceptives. • Sx: puritis, itching, irritation, white cottage cheese-like discharge • Tx: anti-fungal agents (Monistat, Terazol, Mycostatin, Gyne-Lotrimin. Oral: Diflucan
Bacterial Vaginosis • May occur throughout the menstrual cycle • Discomfort or pain usually not associated • Tx: Flagy B.I.D. (available in vaginal gel) • Patients associated with vaginosis should be tested for other STDs
Bacterial Vaginosis • Caused by overgrowth of anaerobic bacteria amd Gardnerella vaginalis • Fish-like odor; pH > 4.7 • Noticeable after sexual intercourse or during menstruation as a result of an increased vaginal pH • Risk fx.: douching after menses, smoking nultiple sex partners, other STDs
Trichomoniais • Second most common STD • May be transmitted by asymptomatic carriers. • May be associated with adverse pregnancy outcomes, PID, cervical neoplasia, infertility • Vaginal discharge may appear thin, yellow-green, frothy, malodorous secretion
Trichomoniais • Causes vaginal irritation, burning, itching • Cervical erythema with multiple small petechiae (strawberry spots) • pH usually > 4.5 • Tx.: treat both partners with Flagyl
Gerontologic Consideratons • Menopause, decreased estrogen • Dry vaginal mucosa thins & atrophies • Leukorrhea (vaginal discharge) • Itching, burning • Management: • Similar to bacterial vaginosis • Estrogen hormones help restore the epithelium
Nursing Care • Relieve discomfort – sitz baths • Reduce anxiety • Prevent reinfection or spread • Patient education: preventive measures • Abstinence from intercourse • Treatment: antibiotics & iontments • Hygiene practices • Reporting symptoms
HPV – Human Papillomavirus • Sexually transmitted • Various HPV strains • 18, 18, 31, 33, 45 result in abnormal pap-smears; cervical dysplagia, risk for cervical cancer • 6, 11 result in condylomata (warts), low risk for cancer • Prevalent among young sexually active females • Tx: topical oint. Tichloroacetic acid, podophyllin (Condylox, Aldara)
Herpesvirus Type 2Herpes Genitalis, Herpes Simplex Virus • Herpetic lesions on external genitalia • Tansmittable STD from wet surfaces • Initial outbreak may be painful • Recurrence are less painful, associated with stress, sunburns, inadequate rest & nutrition, • Complications: spread to buttocks, thighs, eyes.
HPV – Human Papillomavirus • Tx: Valtrex, Zovirax, Famciclovir • HSV-1 (simplex type 1) causes cold sores • HSV 2 (simplex type 2) genital herpes • Varicell zoster or shingles • Estein-Barr virus • Cytomegalovirus (CMV) • Human B-lymphotorphic virus • Sx: papules, macules, vesicular ulcers, blisters on vaginal, cervix, perianal. Glans penis, foreskin & shaft. Flu-like symptoms, malaise, dysuria
Health Problems in Pediatric FemalesAdolescent Reproductive Health Problems
Adolescent Pregnancy • Rates of adolescent births still remain high in the U.S. than other developing countries. • 7 out of 10 adolescent mothers complete high school but are less likely to to to college. • The less familiar an adolescent is with her partner, the less likely it is that they will use contraception during intercourse. • Social factors: low socioeconomics, poverty • Maternal success: participation in programs for pregnant teens, social support systems and a sense of control over one’s life.
Adolescent Pregnancy • Medical aspects. • Risk for complications exist when there is a lack of adequate care • Premature labor, low-birth infants, high neonatal mortality, iron deficiency anemia, fetopelvic disproportion, prolonged labor. • Infants at risk – bacterial infections within the uterus are associated with early preterm delivery (<30 wks)