Download
1 / 67
700 likes | 912 Views
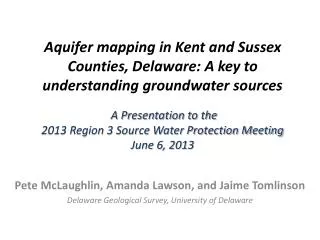
5 - 2 -1- Almost None Let’s Make Delaware’s Kids the Healthiest in the Nation. Obesity Trends* Among U.S. Adults BRFSS, 1985. (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person). No Data <10% 10%–14%. Obesity Trends* Among U.S. Adults BRFSS, 1986.

E N D
5-2-1-Almost NoneLet’s Make Delaware’s Kids the Healthiest in the Nation
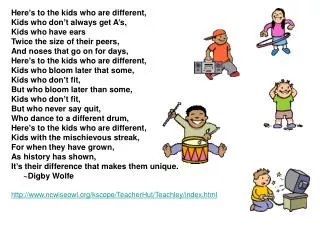
Obesity Trends* Among U.S. AdultsBRFSS, 1985 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14%
Obesity Trends* Among U.S. AdultsBRFSS, 1986 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14%
Obesity Trends* Among U.S. AdultsBRFSS, 1987 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14%
Obesity Trends* Among U.S. AdultsBRFSS, 1988 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14%
Obesity Trends* Among U.S. AdultsBRFSS, 1989 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14%
Obesity Trends* Among U.S. AdultsBRFSS, 1990 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14%
Obesity Trends* Among U.S. AdultsBRFSS, 1991 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19%
Obesity Trends* Among U.S. AdultsBRFSS, 1992 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19%
Obesity Trends* Among U.S. AdultsBRFSS, 1993 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19%
Obesity Trends* Among U.S. AdultsBRFSS, 1994 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19%
Obesity Trends* Among U.S. AdultsBRFSS, 1995 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19%
Obesity Trends* Among U.S. AdultsBRFSS, 1996 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19%
Obesity Trends* Among U.S. AdultsBRFSS, 1997 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% ≥20%
Obesity Trends* Among U.S. AdultsBRFSS, 1998 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% ≥20%
Obesity Trends* Among U.S. AdultsBRFSS, 1999 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% ≥20%
Obesity Trends* Among U.S. AdultsBRFSS, 2000 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% ≥20%
Obesity Trends* Among U.S. AdultsBRFSS, 2001 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
Obesity Trends* Among U.S. AdultsBRFSS, 2002 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
Obesity Trends* Among U.S. AdultsBRFSS, 2003 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
Obesity Trends* Among U.S. AdultsBRFSS, 2004 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
Obesity Trends* Among U.S. AdultsBRFSS, 2005 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
Obesity Trends* Among U.S. AdultsBRFSS, 2006 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
Obesity Trends* Among U.S. AdultsBRFSS, 2007 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
0 What is BMI? A calculation that estimates how much body fat a person has based on his or her weight and height. The BMI formula uses height and weight measurements to calculate a BMI number. Body Mass Index (BMI) = weight(kg)/height (m)2 www.kidshealth.org http://www.cdc.gov/nccdphp/dnpa/bmi/
Trends of Obesity* in Children and Adolescents *BMI > 95th Percentile Data Source: CDC NCHS
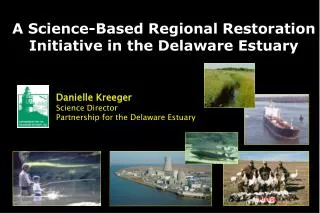
Underweight (BMI < 5th Percentile) 9.5% Obese(BMI > 95th Percentile) 20.5% Overweight(BMI 85th – 94th Percentile) 16.8% Healthy Weight(BMI 5th to <85th Percentile) 53.2% More than one-third of Delaware children and youth are overweight or obese Percentage of Delaware Children and Youth Ages 2-17 by Weight Status Obese (BMI > 95th Percentile) 19.9% Healthy Weight(BMI 5th to <85th Percentile) 60.6% Data Source: Nemours Delaware Survey for Children’s Health, 2006; Note: Data are not adjusted for demographics or co-morbid conditions.
0 What is BMI? A calculation that estimates how much body fat a person has based on his or her weight and height. The BMI formula uses height and weight measurements to calculate a BMI number. Body Mass Index (BMI) = weight(kg)/height (m)2 www.kidshealth.org http://www.cdc.gov/nccdphp/dnpa/bmi/
What is obesity and overweight? • Adults • Overweight = BMI at 25.0 – 29.9 • Obesity = BMI at 30.0 or above • Children: BMI is age and gender specific, so BMI-for-age is the measure used • Overweight = heavier than 85% of children • Obesity = heavier than 95% of children • (using growth charts) • BMI is a good screening tool but it has limitations http://www.cdc.gov/nccdphp/dnpa/bmi/
Consequences of childhood and adolescent obesity • Discrimination • Persistence into adulthood • Abnormal cholesterol • High Blood Pressure • Type 2 diabetes • Liver and Gallbladder Disease • Depression • Anxiety • Asthma • Sleep problems • Earlier maturation • Reproductive problems • Bone complications
Quality of Life • Severely overweight children and adolescents are 5x more likely than healthy weight children to report a low quality of life. • This risk is similar to children diagnosed with cancer Schwimmer et al. Health-related quality of life of severely obese children and adolescents. JAMA. 2003;289:1813-1819. Adapted with permission from NICHQ
Economic Burden • “Obesity-related health expenditures are estimated to have accounted for more than 25% of the growth of health care spending between 1987-2001” -Health Affairs (2004) • “In 2003, an estimated $207 million was spent for health-related expenditures due to obesity in Delaware -Finkelstein (2004) Adapted with permission from NICHQ
What are the causes of obesity? • More calories eaten • Less physical activity • More inactivity
Determinants of weight Energy INTAKE Energy OUTPUT INTAKE OUTPUT OUTPUT INTAKE
What do we know? • No single culprit • No magic bullet • MODERATION—such a boring word! • There are some things we can do…
Children could reduce their risk of preventable disease if: They consumed5 or more servings of fruits and vegetables each day. They reduced screen time to fewer than 2 hours each day. They engaged in a total of at least 1 hour of physical activity each day. They limited drinks with added sugars, specifically soft drinks, non-100% fruit drinks and sports drinks.
What’s a serving? • Fruit: 1 medium whole fruit, ½ cup of cut fruit, • ½ cup 100% juice or ¼ cup of dried fruit • Vegetable: 1 cup of leafy vegetables, ½ cup of raw or cooked vegetables or 100% juice • Fresh, frozen or canned? • It is important to eat a variety of colors
Fruits and vegetables: • May help your stomach feel full. • May decrease the chance of becoming overweight • Decrease chance of chronic disease: • Cancer • Heart Disease Dietary Guidelines for Americans, 2005; Rolls, 2004.
Nationwide, only 21.4% of teens eat 5 fruits and vegetables a day. Source: Youth Risk Behavior Surveillance System, 2007.
Poor dietary patterns are beginning at early stages. • Fruit and vegetable intake in infants and toddlers • does not meet national nutrition recommendations. • French fries are one of three most common vegetables fed to infants 9-11 months. • By 15-18 months, French fries become the most common vegetable consumed. Fox MK, Pac S, Devaney B, Jankowski L. Feeding infants and toddlers study: what foods are infants and toddlers eating? J Am Diet Assoc. 2004;104:S22-S30.