Download
1 / 1
80 likes | 380 Views
Anxiety Screening Test. Please read the following items. Circle YES if an item applies to your more often than not over the past two weeks. Circle NO if an item does not apply to you more often than not over the past two weeks. YES NO “I feel nervous most days.”

E N D
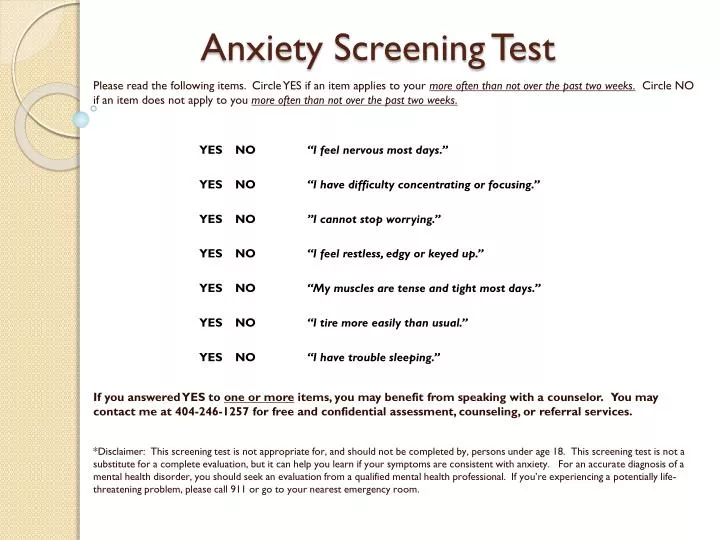
Anxiety Screening Test Please read the following items. Circle YES if an item applies to your more often than not over the past two weeks. Circle NO if an item does not apply to you more often than not over the past two weeks. YES NO “I feel nervous most days.” YES NO “I have difficulty concentrating or focusing.” YES NO ”I cannot stop worrying.” YES NO “I feel restless, edgy or keyed up.” YES NO “My muscles are tense and tight most days.” YES NO “I tire more easily than usual.” YES NO “I have trouble sleeping.” If you answered YES to one or more items, you may benefit from speaking with a counselor. You may contact me at 404-246-1257 for free and confidential assessment, counseling, or referral services. *Disclaimer: This screening test is not appropriate for, and should not be completed by, persons under age 18. This screening test is not a substitute for a complete evaluation, but it can help you learn if your symptoms are consistent with anxiety. For an accurate diagnosis of a mental health disorder, you should seek an evaluation from a qualified mental health professional. If you’re experiencing a potentially life-threatening problem, please call 911 or go to your nearest emergency room.