Download
1 / 10
100 likes | 125 Views
Is the Optic Disc Cupping or Sinking in Glaucoma ? Syed S. Hasnain M.D. Porterville, California, USA Hasnain40@sbcglobal.net.

E N D
Is the Optic Disc Cupping or Sinking in Glaucoma? Syed S. Hasnain M.D. Porterville, California, USAHasnain40@sbcglobal.net • INTRODUCTION: The term ‘glaucomatous cupping’ which was given 150 years ago, implies gradual enlargement of the physiological cup in glaucoma. This presentation is to determine whether the physiological cup is truly enlarging. If not, then what may be occurring to the disc and its physiological cup. • METHOD: This presentation is conveyed in an unconventional approach. Instead of searching for various factors causing glaucoma, three puzzling questions and their answers, based on deductive reasoning, morphology and histology of the glaucomatous discs will be discussed. Author has no financial interest related to this presentation.
Discussion: Three puzzling questions of glaucoma • PUZZLING QUESTION # 1: Why don’t ocular hypertension (OHT) subjects develop glaucoma at high IOPs such as 30mm Hg whereas normal-tension subjects (NTG) develop glaucoma even at normal IOPs (10 – 21 mm Hg)? • PUZZLING QUESTION # 2: Why are the arcuate axons selectively destroyed in early stages, whereas the macular fibers last until the end-stage of glaucoma? • PUZZLING QUESTION # 3: Why can’t glaucoma be halted despite maximally lowering of IOP?
Discussion:Puzzling Questions • PUZZLING QUESTION # 1. Why don’t OHT subjects develop glaucoma at higher range IOPs whereas NTG subjects develop glaucoma even at normal range IOPs? Medical history of 100 glaucoma patients revealed that high-tension patients (HTG) were usually in good health, whereas the NTG patients had cardio-pulmonary and circulatory problems. Interestingly, about 70% of NTG patients were smokers. These findings suggest that NTG may be a systemic disease and glaucoma as a multifactorial disease.Raised IOP is not the only cause of glaucoma. The reason some OHT subjects do not develop glaucoma, may be due to the fact that they may have only one riskfactor (raised IOP)and thus less prone to develop glaucoma.This may answer question #1 as to why some OHT subjects do not develop glaucoma. The more the risk factors present, higher the likelihood of development of glaucoma. • PUZZLING QUESTION #2.Why are the arcuate axons selectivelydestroyed in early stages of glaucoma? Because arcuate scotomas are produced in both HTG and NTG, there should be a common site of injury where the arcuate axons can be selectivelydestroyed in these two types of glaucoma. The arcuate axons can possibly be destroyed at one of three sites: the lamina cribrosa, retina or the junctional area.
Search for Common Site of InjuryCan the arcuate axons within the lamina cribrosa or the retina be selectively destroyed by any cause? • LAMINA CRIBROSA? Unlikely. It is not possible that high IOP, or any other pathology, can selectively destroy only the arcuate axons among the one million or so densely packed axons within the intricate meshwork of the lamina cribrosa. Thus, the lamina cribrosa may not be the primary site of injury. • RETINA? Unlikely. Similar to the case of lamina cribrosa, it is not possible that high IOP, or any other pathology, can selectively destroy only the arcuate axons within the retina in the early stages of glaucoma. Thus, the retina may not be the primary site of injury. Regarding Apoptosis: It is unlikely that our genes are so pre-programmed that they would first predict the impending chronic glaucoma and then initiate apoptosis selectively with only those ganglion cells which serve the arcuate axons. If the lamina cribrosa or retina can’t be the primary and common site of injury, then the border tissue of Elschnig may be the possible site of injury.
Can the border tissue of Elschnig be the common site of injury for HTG and NTG? • Likely. The border tissue of Elschnig lies between lamina cribrosa and the sclera and secures the disc, acting as an ‘O’ ring seal, in the scleral opening. • The border tissue is exclusively supplied by short posterior ciliary arteries having lower pressure compared to the central retinal artery, thus it can be easily compressed by high IOP or directly reduced due to poor systemic circulation. IOP and arterial pressure are opposing forces. Thus, the IOP should be lower than the arterial pressure of the border tissue for its healthy maintenance. • The above circulatory balance would be reversed either due to an increase in IOP or due to reduction in arterial pressure resulting from poor systemic circulation. In the latter scenario, even normal range IOP would become too high and would compress the weak-pressured blood vessels of the border tissue leading to chronic ischemia and atrophy of border tissue and thus sinking of optic disc.
Can the arcuate axons be selectively destroyed if optic disc is sinking? • Likely. As the border tissue of Elschnig which lies between the lamina cribrosa and the sclera atrophies, the lamina would become loose and begin to sink in the scleral canal. Since the disc is usually temporally tilted, the temporal lamina would sink below the scleral edge first. • As the lamina sinks below the scleral edge, all the temporal axons consisting of sup. & inf. arcuate and macular axons (prior to their entry in to lamina), would be stretched (since one end of the axon is still attached to the retina and other to the sinking lamina) and axotomized against the scleral edge simultaneously. However, the arcuate axons being fewer in number, would be depleted earlier, giving rise to double arcuate scotomas, whereas the macular axons being abundant would last until the end-stage of glaucoma. This may answer question #2 as to why are the arcuate axons selectively destroyed in earlier stages and the macular axons last until the end-stage.
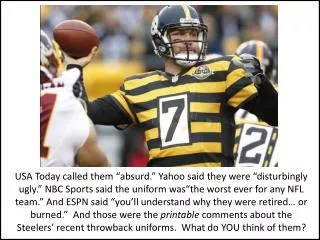
Axotomy of axons in glaucoma Fig. 1. Arcuate axons (blue) and macular axons (black) are being axotomized simultaneously due to disc sinking. Fig. 2. Arcuate axons, being fewer, will be depleted earlier giving rise to arcuate scotomas Fig 3. Hogan & Zimmerman. Intermediate stage. Empty spaces in temporal lamina cribrosa due to disappearance of axons as a result of axotomy. Fig 4. Becker & Shaffer. End-stage glaucomatous disc. Empty crater (unique to glaucoma) due to axotomy of all the axons.
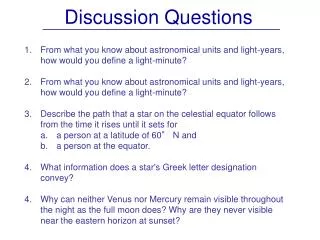
Early to end-stage glaucomatous discs Fig 5. Early stage glaucomatousdisc. Right eye. Splinter hemorrhage at 7 o’ clock. No change in the contour of the physiological cup Fig 6. Advanced stage glaucomatous disc. Left eye. Same patient as in Fig. 5 Fig. 7 Intermediate stage glaucoma. Physiological cup obliterated due to confluence of its normal pallor with the pallor (from destruction) in the rim area. Arcuate scotoma present. Fig. 8 End-stage glaucomatous disc. Marked kinking of the blood vessels due to loss of axons.
What happens as the sinking of the disc continues? • Retinal axons anchor the optic disc in place as roots anchor a tree. As the axons are being axotomized and depleted, the optic disc becomes more loose and sinks further, resulting in severing of additional axons. The axons in the retina are arranged in a way that those originating from the extreme peripheral retina lie deepest and exit from the most peripheral part of the disc (closest to the scleral edge) whereas the axons originating closest to the disc lie most superficial (closest to the vitreous) and exit from the most central part of the disc. • As the disc sinks in its entirety, the deepest prelaminar axons (prior to entry in to lamina), will be stretched and severed against the scleral edge first. As the peripheral axons are being severed, the axons lying in the central part of disc would move towards the periphery to occupy the space vacated by severed axons and thus also axotomised at the scleral edge. This will result in disintegration of the physiological cup. Loss of anchorage of the disc from severed axons will create a self-propagated cascade of loosening and sinking of the disc which would continue until all the axons are axotomized at the scleral edge. Thus, the sinking of the disc would become unstoppable akin to a sinking ship. This may answer question #3 as to why can’t glaucoma be halted despite maximally lowering of IOP.
Conclusion • Since the axons originating closer to disc lie superficial and exit from central part of the disc, these central vision axons should be destroyed first if the physiological cup is truly enlarging. Instead, peripheral vision axons because of their deeper location are destroyed first in glaucoma, consistent with sinking optic disc. • Axons may not being atrophied but axotomized in glaucoma. Axons are being severed prior to their entry into the lamina cribrosa. • The primary and common site of injury may not be the lamina cribrosa but the border tissue of Elschnig for both HTG and NTG. • Glaucoma is a multifactorial disease and NTG a systemic disease. • Continuous severing of prelaminer fibers due to self-propagated sinking of disc would result in progressive thinning of the RNF layer – as revealed by OCT. • Sinking disc may also explain the thinning of macular ganglion cell complex since macular axons are also being axotomised along with both groups of arcuate axons. • Total disappearance of the optic disc and the disc area replaced with an empty crater as revealed by end-stage histology suggests that axotomy (unique to glaucoma), but not atrophy, of the axons may be occurring in glaucoma. Reference: Hasnain SS. Scleral edge, not optic disc or retina is the primary site of injury in chronic glaucoma. Medical Hypotheses. 2006;67;1320-1325