Download
1 / 29
290 likes | 450 Views
Measuring the Prevalence of Prenatal Alcohol Exposure. Shannon Lange, Kevin Shield, Gideon Koren, Jürgen Rehm, & Svetlana Popova. Presented by Shannon Lange, MPH. Presented at Public Health 2014 Canadian Public Health Association. INTRODUCTION.

E N D
Measuring the Prevalence of Prenatal Alcohol Exposure Shannon Lange, Kevin Shield, Gideon Koren, Jürgen Rehm, & Svetlana Popova Presented by Shannon Lange, MPH Presented at Public Health 2014 Canadian Public Health Association
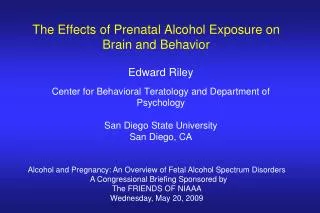
INTRODUCTION • Prenatal alcohol exposure is an established cause of Fetal Alcohol Spectrum Disorder (FASD) • FASD is a non-diagnostic umbrella term used to characterize the full range of damage caused by prenatal alcohol exposure • FASD is associate with a broad array of physical defects and cognitive, behavioural, emotional, and adaptive functioning deficits, as well as congenital anomalies
INTRODUCTION (Con’t) • FASD includes the following 4 diagnoses: • Fetal Alcohol Syndrome (FAS), • Partial Fetal Alcohol Syndrome (pFAS), • Alcohol-related Neurodevelopmental Disorder (ARND), and • Alcohol-related Birth Defects (ARBD)
INTRODUCTION (Con’t) FAS is the most severe and visibly identifiable form of FASD Epicanthic folds Low nasal bridge Short nose Short midface Thin upper lip Small head circumference Short palpebral fissures (short eye openings) Indistinct/smooth philtrum (groove above the lip)
INTRODUCTION (Con’t) FAS is a leading cause of brain damage in newborns 5-day-old infant (control) 5-day-old infant with FAS Adapted from Clarren, 1986
INTRODUCTION (Con’t) • Identification of infants exposed to alcohol in utero is crucial, as it can: • Lead to close monitoring of his/her development, • Facilitate early FASD diagnosis and the implementation of timely interventions • Facilitate early recognition and intervention for affected siblings • Prevent subsequent alcohol-exposed births • Reduce the occurrence of secondary disabilities
INTRODUCTION (Con’t) How Can We Ascertain Prenatal Alcohol Exposure? There are two commonly used methods: Maternal self-reports and Meconium testing
INTRODUCTION (Con’t) • Maternal Self-reports • Simple and inexpensive • Often under-reported for a variety of reasons • Vulnerable to biases (social desirability bias and recall bias) • Fear of consequences (child may be taken away, stigmatization) • Guilt and shame • Thus, maternal self-report are often unreliable • Necessitating the use of an unbiased biomarker to identify those at risk for FASD
INTRODUCTION (Con’t) • Meconium Testing • Detection of fatty acid ethyl esters (FAEE; products of non-oxidative ethanol metabolism), above laboratory cut-points in meconium • A novel and established biomarker of prenatal alcohol exposure in the 2nd and 3rd trimesters • Cumulative FAEE concentrations exceeding 2.0 n▪mol/g is indicative of 7+ drinks/week • or 5+ drinks/occasion (“binge” drinking) • High sensitivity (84.2%) and • specificity (83.3%)
OBJECTIVE • The objective of the study was two-fold: • 1) To compare the prevalence of prenatal alcohol exposure using maternal self-reports with the results of meconium testing, and • 2) To quantify the disparity in the estimates obtained using these two methods
METHODS • There were three steps involved in the methodology of this study: • Systematic Literature Review • Meta-analysis • Meta-regression
METHODS (Con’t) • Systematic Literature Review • Performed in multiple electronic bibliographic databases to identify studies published prior to January 2013 that have estimated the prevalence of prenatal alcohol exposure (at any level and at any point of time) using both maternal self-reports and meconium testing
METHODS (Con’t) • Meta-analyses • Performed using the Mantel-Haenszel method, assuming a random-effects model • Prevalence estimates were transformed using a double arcsine transformation so that the data followed a normal distribution
METHODS (Con’t) • Meta-regression • A random effects meta-regression was performed to test for a difference in the prevalence estimates of prenatal alcohol exposure as measured by maternal self-reports and those obtained by meconium testing • A logit regression (using log odds transformed prevalence estimates) was used
RESULTS • 8 articles were retained all together Figure 1. The prevalence of prenatal alcohol exposure obtained using maternal self-reports versus meconium testing and the pooled prevalence estimate
RESULTS • 8 articles were retained all together Figure 1. The prevalence of prenatal alcohol exposure obtained using maternal self-reports versus meconium testing and the pooled prevalence estimate
RESULTS (Con’t) • Meta-regression • The prevalence of prenatal alcohol exposure as measured by meconium testing was 4.26 (95% CI: 1.34 to 13.57) times the prevalence of prenatal alcohol exposure as measured by maternal self-reports (p = 0.021)
DISCUSSION • Limitations • Studies used difference instruments/methods to obtain self-reported data, each with its own sensitivity and specificity • The majority of studies did not specify the time period captured by the exposure assessment • Thus, self- reported data may not be reflective of the same time period as the meconium testing data
DISCUSSION (Con’t) • Implications • Health care professionals should be aware of the under-reporting of prenatal alcohol exposure by maternal self-reports • If such under-reporting is not adjusted for, a number of prenatally alcohol-exposed infants and women who are at-risk of consuming alcohol during pregnancy are not being identified as such
DISCUSSION (Con’t) • Recommendations • Education about the detrimental effects of prenatal alcohol exposure must be provided to all women of childbearing age; • Enhance access to substance abuse treatment programs for the mothers of children with FASD; • Increase the effectiveness of substance abuse treatment programs for women of childbearing age (in order to prevent the occurrence and/or recurrence of FASD within families);
DISCUSSION (Con’t) • Recommendations (Con’t) • Universal screening and provision of brief interventions, where appropriate, to all pregnant women should be established; and • Improving data collection on prenatal alcohol exposure is necessary, especially for at-risk populations
THANK YOU! Remember: When you drink, so does your child Email: shannon.lange@camh.ca
RESULTS (Con’t) Meta-analyses Figure 2. Forest plot of the prevalence of prenatal alcohol exposure as measured by maternal self-reports
RESULTS (Con’t) Meta-analyses Figure 3. Forest plot of the prevalence of prenatal alcohol exposure as measured by meconium testing
METHODS (Con’t) • Inclusion/Exclusion Criteria • Articles were retained if they: • i) Consisted of original, quantitative research on human participants published in a peer- reviewed journal; and • ii) Obtained a measurement of maternal alcohol use during pregnancy via self-reports (e.g., interview, questionnaire, etc.) in combination with meconium testing for FAEE with a pre-defined cumulative cut- point
DISCUSSION (Con’t) • Limitations (Con’t) • Meconium testing cannot ascertain prenatal alcohol exposure during the 1st trimester, nor can it detect consumption of less than 7+ drinks per week and/or less than 5 drinks per occasion (binge drinking) during the 2nd and 3rd trimesters • Variations in the laboratory methods for testing meconium for the presence of FAEE (e.g., extraction methods, analytical strategies)