Download
1 / 10
100 likes | 309 Views
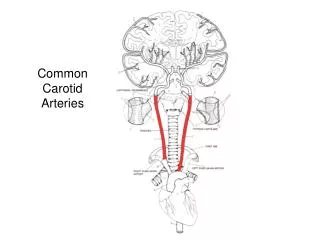
University Clinical Center Tuzla Clinic for Cardiovascular Diseases Department of Cardiovascular Surgery. Pseudoaneury s m of the internal carotid artery caused by a gunshot wound (Case Report) Tuzla, 26.05.2010.g.

E N D
University Clinical Center Tuzla Clinic for Cardiovascular Diseases Department of Cardiovascular Surgery Pseudoaneurysm of the internal carotid artery caused by a gunshot wound (Case Report) Tuzla, 26.05.2010.g
A 22 years old man was admitted in the ICU because of a gunshot wound he suffered on October, 17th 2009. At the moment he was admitted he was conscious and breathing spontaneously. His pupils were isocoric but enlarged. His heart action was tachycardic, CP=120 1/min, blood pressure 160/107 mmHg. The breathing sound was diffuse quiet. His extremities were cold, the pulsations of the arteries on the upper and lower extremities were filiform.
On the left side of the lower jaw the entry hole of the gunshot wound was determined. The exit hole was on the right side of the neck. In the area of the mental protuberance there was an oedema and a haemathoma placed on the bottom of the oral cavity. An emergent CT scan of the head and neck was done. On that scan a gunshot wound was established that was spreading from left and forward to the right and back. We also established a multifragmentar fracture of the lower jaw with an enlarged soft tissue oedema. In the area of the upper jaw's alveolar processus a metal like density area was described.
On October 19th, a CT angiography scan of the head and neck vessels was provided. A pseudoaneurysm of the common and internal carotid artery was diagnosed that was also compressing the internal iugular vein. In the postoperative course the patient was septic, intubated. His general condition was severe. After the septicemia had been stabilised and the patient was extubated the paseudoaneurysm of the internal carotid artery suddenly ruptured with a massive bleeding. A second emergency surgery in terms of haemostasis was implemented. During the surgery a serious wound infection was established.
After clinical and laboratory finding were stabilised we decided to perform a third surgery which was done on November, 21st 2009. Resectio pseudoaneurysmae a.carotis communis et a.carotis internae l.dex. Reconstructio a.carotis communis et a.carotis internae l.dex cum interpositum (v.saphena magna graft). Ligatura a.carotis externae l.dex. Redon drainage.
From the third surgery on, the postoperative cours was proceeding without any further complications. On the second postoperative day the patient was discharged from the ICU and he was moved to the department of cardiovascular surgery where he was treated conservative. He was discharged home on 03.12.2009. We followed up the patients health status in regular time intervals. The findings of a control CT angiography that was performed 15.02.2010 was regular beside the ligation of the external carotid artery.