Download
1 / 28
280 likes | 311 Views
Study on root canal morphology in Ghanaian population, analyzing variations in canal numbers in maxillary premolars, using radiographs.

E N D
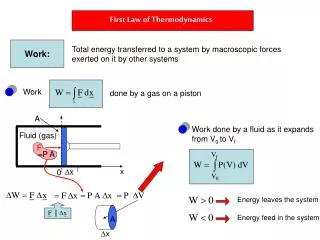
Radiographic In-Vivo Determination of the number of Canals in maxillary premolars of a Ghanaian population Ampofo P.,NyakoE.A., Blankson P., and Konadu A. University of Ghana School of Medicine and Dentistry, Accra, Ghana Korle-Bu Teaching Hospital, Accra, Ghana
OUTLINE • Background • Introduction • Objectives • Materials and Methods • Results • Discussion • References
Mr. Kpodzro presented at the Emergency Unit with a 4-day history of swelling in the right maxillary region which gradually increased in size. • He was subsequently referred to the Dental department where thorough investigation was done. • Hb-10.8 g/dL; WBC- 10.30 x 109/L; Vitals and other results were grossly normal • He had apparently been seen by a Dentist 3-months prior to presentation where a root-canal was done on the second upper premolar which was confirmed on X-ray.
INTRODUCTION • Back to Basics • The Concept of Reversible vrs Irreversible Pulpistis
WHAT IS ROOT CANAL THERAPY • A sequence of treatment for the infected pulp of a tooth which results in the elimination of infection and the protection of the decontaminated tooth from future microbialinvasion.
It is evident that the root canal varies with size, shape and number of roots in different teeth,1 it is a known pertinent consideration in endodontics. • Successful General dental procedures and Root canal therapy in particular requires a thorough knowledge of tooth anatomy and root canal morphology2,3
With a variation in the number of canals4, the maxillary premolars remain one of the challenging teeth to treat endodontically, • Also because of the direction and longitudinal depressions of the roots, the various pulp cavity configurations, and the difficulties in visualizing the apical limit by radiographs 5
The Objective? • Many factors contribute to differences in canal morphology4 but largely influenced by ethnic background, age and gender of the populations studied5,6,7,8 • Despite copious data on several populations worldwide, data is scarce for Ghana. • This study thus describes a clinical survey by use of radiographs to determine the number of canals in maxillary premolars in a Ghanaian population.
Materials And Methods • Four hundred and two (402) participants were selected from patients who had opted for, and were referred to the Restorative Dentistry Department of the University Ghana School of Medicine and Dentistry for endodontic treatment of maxillary premolar from January 2012 till December 2015. • Preoperative radiographs were taken for evaluation (root morphology, number of canals, and periapical status).
The teeth that were included in this study were those teeth that required nonsurgical endodontic treatment. • The included teeth were free of root resorption, had no calcifications or open apices and no retreatment cases were included in the study, patients who defaulted treatment at any point were also excluded. • Consent was sought from each patient.
The teeth included were both clinically and radiographically examined by three specialists with more than 10 years of experience in endodontics and all patients operated on by the same certified Dental Surgeons • The endodontic procedures undertaken were as follows: local anesthesia consisting of 2% Lidocaine in 1:100,000 adrenaline was administered by infiltration.
After the contents of the pulp chamber were removed, a sharp endodontic explorer was used to explore the developmental grooves carefully to locate the orifices of the canals. Copious amount of 2.5% sodium hypochlorite irrigation was used. • Pulp tissue was extirpated using barbed broaches and the canals were flared with gates glidden burs. • Examination of the floor of the pulp chamber to locate canals orifices was done using 3.5 high resolution magnification loupes (Azdent). • The number of root canals in the maxillary first and second premolars was recorded with correlated folder numbers, age and gender. The data was analyzed
RESULTS • A total of 402 patients were used in the study. 239 of these were females and 163 males, representing 59.45% and 40.55% respectively. • Of the total number of teeth used, 160 were maxillaryfirst premolars while 242 were maxillary second premolars. • The age ranged from 16yrs to 82yrs with a mean age of 40yrs.
DISCUSSION • Determination of pulp anatomy generally fall within In-vivo (Clinical) or In-vitro studies. • While in-vitro methods encompass teeth sectioning of extracted or cadaveric teeth, to apply dyes, contrasting media or scanning electron microscopy for analysis,6,7 • Clinical methods on the other hand uses Anatomy studies, exploration, high resolution CT, Visualization endogram, Fibreoptic endoscopy, magnetic resonance imaging and radiographs, which our study employs6,8
While Maxillary first premolars are considered to have two canals, Maxillary second premolar are generally considered to have one canal.9,10,11,12 • In the present study, the latter had one canal in 24.7% of cases. This is at variance with the studies of Green9 and Vertucci et al. 10 in which the maxillary second premolars was reported to have one canal in 72% and 75% of cases respectively.
Like other anatomical features, it is natural to assume racial and ethnology influences on dental morphology differences. • It has been observed that different populations show distinctive variations of tooth morphology.18 • Our study’s 95.4% and 75.3% finding for the first and second maxillary premolars respectively is much higher than reported in Asian studies in Singapore 20 and Sichuan province, China 21
In 1969, Weine et al.22,23 provided the first classification of more than one canal system in a single root and used the mesiobuccal root of the maxillary first molar as the type specimen. • Vertucci further studied the canal anatomy extensively establishing eight different classification of pulp anatomy.24,25 which the authors propose for the curriculum in Ghana
Type I: A single canal extends from the pulp chamber to the apex • Type II: Two separate canals leave the pulp chamber and join short of the apex to form one canal • Type III: One canal leaves the pulp chamber and divides into two in the root; the two then merge to exit as one canal • Type IV: Two separate, distinct canals extend from the pulp chamber to the apex • Type V: One canal leaves the pulp chamber and divides short of the apex into two separate, distinct canals with separate apical foramina • Type VI: Two separate canals leave the pulp chamber, merge in the body of the root, and redivide short of the apex to exit as two distinct canals • Type VII: One canal leaves the pulp chamber, divides and then rejoins in the body of the root, and finally redivides into two distinct canals short of the apex • Type VIII: Three separate, distinct canals extend from the pulp chamber to the apex
CONCLUSION • The incidence of two canals in maxillary premolars of the Ghanaian population is very high. • Students and Clinicians should be made aware of this extreme variation so that further inspection and careful interpretation of preoperative radiographs is done for success in endodontic therapy, especially of the maxillary second premolar.
SUMMARY • This study was done to determine the number of canals in maxillary premolars in a Ghanaian population. • 402 participants were selected from patients who were referred for endodontic treatment of maxillary premolars. These consisted of 239 females (59%) and 163 males (41%). The teeth included in the study were examined clinically and radiographically for the number of root canals using magnifying loupes. • 95.4% of the maxillary first premolars had two canals while 75.3% of the maxillary second premolars also had two canals. There was no significant association between gender and the number of canals in each premolar.
REFERENCE • Ingle, John Ide & Bakland, Leif K & Health Communication Network 2002, Endodontics, 5th ed, B C Decker, Hamilton, Ont. ; London • D'Souza R. Development of the pulpodentinal complex. In: Hargreaves K, editor. Seltzer and Bender's Dental Pulp. Chicago, Ill, USA: Quintessence Books; 2002. • Cleghorn B, Christie W, Dong C. Root and root canal morphology of the human mandibular first premolar: A literature review. J Endod. 2007;33:509–16. [PubMed] • Jayasimha Raj U, Mylswamy S. Root canal morphology of maxillary second premolars in an Indian population. Journal of Conservative Dentistry : JCD. 2010;13(3):148-151. doi:10.4103/0972-0707.71648. • Pecora JD, Sousa Neto MD, Saquy PC, Woelfel JB. Root form and canal anatomy of maxillary second premolars. Braz Dent J. 1992;3:81–5. [PubMed] • Author/Editor: GargNisha , GargAmit , Speciality:Conservative Dentistry and Endodontics • Jayasimha Raj U, Mylswamy S. Root canal morphology of maxillary second premolars in an Indian population. J Conserv Dent. 2010;13:148–51. [PMC free article] [PubMed] • Nur BG, Ok E, Altunsoy M, Aglarci OS, Colak M, Gungor E. Evaluation of the root and canal morphology of mandibular permanent molars in a south-eastern Turkish population using cone-beam computed tomography. European Journal of Dentistry. 2014;8(2):154-159. doi:10.4103/1305-7456.130584.
9. Green D. Double canals in single roots. Oral Surg Oral Med Oral Pathol 1973; 35: 689-96. 10. VertucciF, Seelig A, Gillis R. Root canal morphology of the human maxillary second premolar. Oral Surg Oral Med Oral Pathol 1974; 58 456-64 11. G. Cantatore, E. Berutti, and A. Castellucci, “Missed anatomy: frequency and clinical impact,” Endodontic Topics, vol. 15, no. 1, pp. 3–31, 2006. 12. L. J. Buhrley, M. J. Barrows, E. A. BeGole, and C. S. Wenckus, “Effect of magnification on locating the MB2 canal in maxillary molars,” Journal of Endodontics, vol. 28,no. 4, pp. 324–327, 2002. 13. ChimaO. Number of root canals of the maxillary second premolar in Nigerians. Odonto-stomatolTrop 1997; 78 : 31-2 14. PecoraJD, Sousa Neto MD, Saquy PC, Woelfel JB. In vitro study of root canal anatomy of maxillary second premolars. Braz Dent J 1993; 3: 81-5. 15. WengXL, Yu SB, Zhao SL, Wang HG, Mu T, Tang RY. Root canal morphology of permanent maxillary teeth in the Han nationality in Chinese Guanzhong area: A new modified root canal staining technique. J Endod 2009;35:651-6. 16. Pineda F, Kuttler Y. Mesiodistal and buccolingualroentogenic investigations of 7,275 root canals. Oral Surg. 1972;33:101–10. [PubMed] 17. RwenyonyiCM, Kutesa A, Muwazi L, Buwembo W. Root and canal morphology of maxillary first premolar teeth in a Ugandan population. Open J Stomatol 2011;1:7-11. 18. Al-NazhanS, Al-Daafas A, Al-Maflehi N. Radiographic investigation of in vivoendodontically treated maxillary premolars in a Saudi Arabian sub-population. Saudi Endod J 2012;2:1-5.
19. Ahmad IA. Root and root canal morphology of Saudi Arabian permanent dentition. Saudi Endod J 2015;5:99-106. 20. LohHS. Root morphology of the maxillary first premolar in Singaporeans. Aust Dent J 1998;43:399-402. 21. Deng D, Zhang M, Wu W. The morphology study of root canal system of permanent teeth. Sichuan J Anat 2004;12:226. 22. WeineFS, Healey HJ, Gerstein H, Evanson L. Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance. Oral Surg Oral Med Oral Pathol. 1969;28:419–25. [PubMed] 23. GulabivalaK, Aung TH, Alavi A, Ng YL. Root and canal morphology of Burmese mandibular molars. IntEndod J. 2001;34:359–70. [PubMed] 24. AwawdehLA, Al-Qudah AA. Root form and canal morphology of mandibular premolars in a Jordanian population. IntEndod J. 2008;41:240–8. [PubMed] 25. VertucciFJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10:3–29 26. SertS, Bayirli GS. Evaluation of the root canal configuration of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod. 2004;30:391–8. [PubMed]