Download
1 / 29
300 likes | 333 Views
Explore the complex issues surrounding low back pain in primary care, unraveling its challenges and providing effective management strategies. Delve into the epidemiology, differential diagnosis, imaging guidelines, and referral protocols for optimal patient care. Learn how to navigate the intricacies of low back pain and empower patients to make informed healthcare decisions. Join us in untangling the Gordian knot of low back pain management.

E N D
Back Pain in Primary Care: Untangling the Gordian Knot W. Lee Warren, MD, FACS Medical Director Advantage Orthopedics and Neurosurgery Casper, Wyoming
The Gordian Knot • 333 B.C. Alexander the great marched his army into the Phrygian capital of Gordium in modern day Turkey. • Upon arriving in the city, he encountered an ancient wagon, its yoke tied with what one Roman historian later described as “several knots all so tightly entangled that it was impossible to see how they were fastened.”
The Gordian Knot • Phrygian tradition held that the wagon had once belonged to Gordius, the father of the celebrated King Midas. An oracle had declared that any man who could unravel its elaborate knots was destined to become ruler of all of Asia. • According to the ancient chronicler Arrian, the impetuous Alexander was instantly “seized with an ardent desire” to untie the Gordian knot. After wrestling with it for a time and finding no success, he stepped back from the mass of gnarled ropes and proclaimed, “It makes no difference how they are loosed.” He then drew his sword and sliced the knot in half with a single stroke.
Is Low Back Pain is the Gordian Knot of our Time? The Gordian Knot is often used as a metaphor for an intractable problem (disentangling an "impossible" knot) solved easily by finding a loophole or thinking creatively ("cutting the Gordian knot"): Turn him to any cause of policy,The Gordian Knot of it he will unloose,Familiar as his garter — Shakespeare, Henry V, Act 1 Scene 1. 45–47
Is Low Back Pain is the Gordian Knot of our Time? • Is LBP an intractable problem, an un-solvable puzzle? • Does it really, “Make no difference how it is loosed?” • Is there a “single stroke” to cut the knot? • Why does Casper lead the nation in spinal fusion surgeries per capita? • How can surgeons and primary care doctors manage this difficult problem, work better together, and help their patients make the best decisions possible for their health care?
To answer those questions… more questions! • Why do so many people have back surgery? • When SHOULD people have back surgery? • When do people REALLY need fusion surgery?
Goals of this Lecture • Review the epidemiology and economics of low back pain • Review the differential diagnosis of low back pain and Redflag symptoms and signs that requireimmediate work up • Discuss when and how to image low back pain • Discuss when to refer to subspecialist • A word about stem cells
Low Back PainEpidemiology and Economics • Lifetime incidence of acute low back pain is 60-90%, annual incidence 5% of population. • 2nd to 5th chief complaint in primary care clinics • 90% resolve within 6-12 weeks • Chronic low back pain-13 million physician visits annually • Back pain is the number one cause of disability in U.S. for people under 45 years. • WHO estimates $100 billion/year USA cost
Low Back Pain: Cold Hard Facts • Increased availability of imaging and surgical treatments have NOT reduced the economic burden of this disorder, “A symptom in search of a disease.” JAMA • Since >90% resolve in a few weeks, early imaging is NOT recommended in absence of red flag symptoms (Meaningful use standard is six weeks) • Early imaging does NOT change outcome, but does lead to increased procedures performed (NASS) • Casper WY leads the USA in spinal fusions per capita (New York Times)
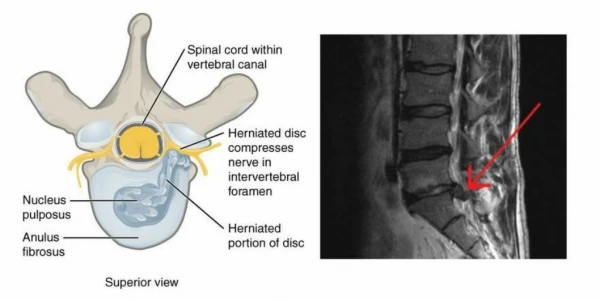
Case 1 • 48 year old oil field worker with stiffness and soreness in the low back one day after welding on a rig. • Sharp pain, 8/10 with bilateral leg weakness. Complains of numbness in the groin region. No other symptoms. • No PMH, NKDA, No PSH • ROS: No hx of LBP, no recent fever, infection, weight loss, cancer, fever, abdominal complaints. • Social: Ex smoker 5 pack-yrs., no EtOH, no other drugs. Hobbies are hunting, horseback riding.
Case 1 • Exam: 5’9”, 195, 112/82, P-88, RR-14. • W/D fit appearing muscular male ambulates with difficulty, slow guarded gait, prefers to stand. • HEENT, Heart, Lungs, WNL. • Abdomen-Soft flat, non-tender, without rebound or bruit, no CVAT or hernia genitalia WNL. • Lumbar spine-flat lordosis, spasm, with L/S junction TTP, and ROM limited to few degrees. • Neuro-Reduced touch, and sharp dull, bilaterally L4-S1, global weakness, 4/5 multiple myotomes.
Case-Mr. J.M. • Other exam findings? • Tests? • Radiographs? • Imaging? • Diagnosis? • Referral?
Red Flags • A focused medical history, work history and physical exam. • Evaluation of underlying conditions, including sources of referred symptoms in other parts of the body. • Frequency, intensity and duration of complaints. • Aggravating and relieving factors. • History and Physical findings that raise suspicion for serious underlying disorders= Red Flags
Red Flags-for back pain • Age over 50. • Unexplained weight loss, history of cancer. • Persistent fever; recent bacterial infection. • History of intravenous drug use. • Immunocompromized. • Urinary or stool incontinence/urinary retention. • Trauma. • Neurologic deficit, weakness.
Case Ms. T.W. • 48 year old female financial services secretary presents with a three week history of bilateral low frequent back pain 6/10 without radiation. The cause of the pain is unknown but is worsened by prolonged sitting. She feels unable to do her walking program-requests MRI to “find out what is wrong”. • PMH: Depression, r/o fibromyalgia per family physician-rheumatic work up negative. • PSH: TAH-BSO 1 year ago. Bilateral CTS releases. • ROS: Negative for F/C, constitutional symptoms, head or neck pain, -IBS, -chronic fatigue, +weight gain • Social Hx: Divorced, college grad, resides with two teenagers, Ex. ½ ppd smoker x 8 yrs, 3 glasses of wine/week.
Pain • IASP “Unpleasant sensory and emotional experience associated with actual or potential tissue damage”. • Need to address emotional component of pain fist…then understand the actual or potential tissue damage. • Pain is subjective…interacting with the limbic system with modulation of pain…many potential sources of potential pain in the low back…muscles, facets, discs, nerve impingement.
Common Back Pain Misconceptions • “I injured my disc lifting something heavy at work. That’s why my disc is bulging.” • “My 'degenerated’ disc is causing my pain.” • “Because I have back pain, I should stay away from work.” • “Back pain often leads to permanent impairment or disability.” • “Because I have back pain, I will need permanently modified work.” • “The radiology report said my back is screwed up.”
Common Back Pain Misconceptions • I should rest until my back pain goes away. • My back pain means I have really significant biological damage or disease. • X-rays, CT, and MRI can always identify the cause of pain. • Back pain will usually be cured by medical treatment. • My PCP said you’d take over my pain meds.
MRI Imaging • MRI is very sensitive, providing excellent view of soft tissues and vertebrae. • Limitation is lack of specificity—false positives, “UBO’s” • NEJM study of 98 asymptomatic individuals between 20 and 80 years (average 42.3). • 52% had a bulge at least one level. • 27% had a protrusion. • 1% had an extrusion • Patients read reports, surgeons operate on patient’s beliefs Jensen MC, et. Al, MRI of the Lumbar Spine in People without Back Pain, NEJM, 1994, Jul 14, 331(2): 69-73.
Medication Management • APAP and non-selective NSAIDS Recommended for acute low back pain as a first line to allow activity and functional restoration. • Associated with NNT of 2-3 for a 50% reduction in pain. • Muscle relaxants are an alternative. • Use opioids uncommonly. In severe cases should use up to 2 weeks max-in the acute phase only, with caveats. • AON does not prescribe narcotics pre-op.
Back Pain Facts • Internists and other primary care physicians will need expertise in the E & M of acute back pain. • Providers may have a positive impact on improving outcomes, reducing symptoms, and improving functional recovery. • Excessive over-medicalization, and disability are not supported by the evidence in the majority of cases. These outcomes can be prevented with close attention to patient’s history, detailed exam, and multidisciplinary approach to management.
When to Refer to Neurosurgery/Spine Surgery • Any patient with symptoms >6 weeks in spite of physical therapy/steroids, etc. • Any patient with red flags or neurologic deficit • Any patient your gut tells you to refer- we’ll help you • The new AON will strive to become the region’s leader in managing these patients in a multidisciplinary fashion. • Our plan involves developing standards and solid data analysis to determine what’s working, how to reduce the number of fusion procedures done in Casper, and how to maximize outcomes so we can finally cut the Gordian Knot of low back pain.
Questions? Call me: 334-324-2288 Send me an email, lee@drleewarren.com (Ill write back) 334-324-2288 Sign up for my newsletter at www.wleewarrenmd.com