Download
1 / 19
190 likes | 384 Views
SPECIALTY HOSPITALS: FOCUSED FACTORIES OR CREAM SKIMMERS?. Presented to the HSC Specialty Hospitals Conference April 15, 2003 Kelly J. Devers, Ph.D. Objectives. Prevalence and Characteristics Drivers of Development Vital Signs to Monitor Policy Implications.

E N D
SPECIALTY HOSPITALS: FOCUSED FACTORIES OR CREAM SKIMMERS? Presented to theHSC Specialty Hospitals Conference April 15, 2003 Kelly J. Devers, Ph.D.
Objectives • Prevalence and Characteristics • Drivers of Development • Vital Signs to Monitor • Policy Implications
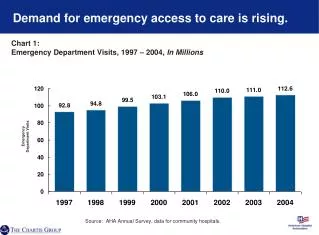
Number of Specialty Hospitals Increasing Rapidly • Since 1997, 11 freestanding specialty hospitals have opened or are planned in the 12 CTS site visit communities • Cardiac and orthopedic procedures are the most common focus • Over 50 specialty hospitals are estimated to exist nationally and more are underway
Key Characteristics • Ownership arrangements are diverse • National for-profit firms, general hospitals, physicians, or combinations of these groups • Partial physician ownership is common • Scope of services provided varies • Emergency department • Other services
Drivers of Development • Relatively high reimbursement for some procedures • Physicians’ desire to increase control over decisions affecting their work environment • Physicians’ desire to increase their income • Higher productivity increases income from professional fees • Facility fees can add additional income
Indianapolis: A Case Study • In the last two years, 5 specialty hospitals have been opened or planned • Building boom began when specialists threatened to partner with MedCath • 2 joint ventures; 2 solely owned by general hospitals; and 1 solely owned by physicians • All add some new bed capacity
General Hospitals’ Response • Aggressively compete • Establish own specialty hospital to avoid or counter physician defection • Fight back • Economic credentialing of physicians • Discourage plans from contracting with competing specialty hospitals • Joint venture with physicians • Keep at least “half a loaf”
Focused Factories’ Promise • Improve quality and reduce costs by: • Performing a high volume of select procedures • Building optimal facilities for delivering these select procedures • Selecting the best staff and motivating physicians through ownership • Innovating and continuously improving care delivery
Concerns about Cream-Skimming • Specialty facilities might succeed primarily by selecting: • Better paying services • Better paying patients • Relatively healthy patients
Will Demand Increase Enough to Fill Additional Capacity? • Proponents say yes • If not in local market, they can draw patients from other markets • Critics say no • Specialty hospitals will have to take patient volume from general hospitals
Vital Signs to Monitor • Quality • Cost and price • Access
Quality • Specialty hospitals can use focused-factory techniques to improve quality • Yet specialty hospitals may lead to similar or poorer quality by: • Spreading the same volume over more facilities • Inappropriate utilization of services • Not providing a full range of services
Per-Case Costs • Specialty hospitals can use the same focused factory techniques to achieve lower per-case costs • Critics contend specialty hospitals may lead to similar or higher per-case costs by: • Spreading the same volume over more facilities • Creating excess capacity (i.e.,empty beds)
Total Costs • Total costs may stay the same or fall because: • Per-case costs could decline enough to offset any utilization increases • Yet specialty hospitals may increase total costs by: • Creating excess capacity • Over-utilization of services • General hospitals increasing prices for other services
Price • More competitors and capacity will spur greater price competition • But price competition may be constrained by: • Large, general hospital systems’ negotiating rates for owned specialty facilities and... • …discouraging plans from contracting with competing facilities
Access • Improved access to specialty services, particularly for some types of patients • But general hospitals risk losing ability to provide less-profitable but essential services • Some services may be closed or scaled back • May have greater impact on Medicaid and uninsured patients
Policy Challenge • Allow competition and innovation, while guarding against potential problems
Policy Options • Revise Medicare payment policy • Develop new ways to preserve access to essential services besides cross-subsidies • Regulate specialty hospitals • E.g., Stark, certificate-of-need, quality and patient-safety standards
HSC, FUNDED EXCLUSIVELY BY THE ROBERT WOOD JOHNSON FOUNDATION, IS AFFILIATED WITH MATHEMATICA POLICY RESEARCH, INC.