Download
1 / 24
250 likes | 299 Views
Learn about α-Adrenergic Blockers, Phenoxybenzamine, Phentolamine, α1-blockers, Yohimbine, β-Adrenergic Blockers, Propranolol, Nadolol, Timolol, Acebutolol, and more. Understand their mechanisms, side effects, and therapeutic applications in various conditions.

E N D
α-Adrenergic Blocking Agents • Affect BP-------decreased PVR------- reflex tachycardia
Phenoxybenzamine • Nonselective, irreversible, noncompetitive • Decrease PVR ----- reflex tachycardia • α2 block--------- increased CO ????? • Pretreatment with phenoxybenzamine followed by Epi??? • Used in Pheochromocytoma (before surgery or inoperable tumor) & in Raynaud disease • SEs: postural hypotension, nasal stuffiness, NV, sexual disturbances, & reflex tachycardia
Phentolamine • Competitive, nonselective α-blocker (4 hrs) • Postural hypotension • Reflex cardiac stimulation • CI in patients with coronary artery disease • Used locally to prevent T necrosis • Used for short term treatment of Pheochromacytoma • Useful in hypertensive crisis due to clonidine abrupt withdrawal & in (tyamine + MAOIs)
Prazocin, Terazocin, Doxazocin, Tamsulosin, Alfuzocin • Selective, competitive α1-blockersuseful in hypertension • Tamsolosin & alfuzocin used in benign prostatic hyperplasia (BPH) • Metabolized & excreted in urine except for doxazocin • Doxazocin have long duration of action • Decreases PVR, BP (venous & arterial effect) • Minimum effect on CO, RBF, & glomer. Filtration rate • Tamsulosin has the least vascular effect (α1B) & higher effect on prostate (α1A)
α-blockers cont. • 1st dose effect • Modest improvement in lipid profile & glucose metabolism in hypertension • SEs: dizziness, lack of energy, headache, orthostatic hypotension, Floppy iris syndrome • α-blockers + vasodilators (ex. Nitrates or PDEIs)??? • Sexual dysfunction
Yohimbine • Selective, copmetetive α2-blocker • Treat erectile dysfunction • Increases CNS sympathetic out flow • CI in CVDs, psychiatric conditions & renal dysfunction
β-Adrenergic Blocking Agents • Competetive, nonselective β1 & β2 • Differ in intrinsic sympathomimetic activity, CNS effects, blockade of sympathetic Rs, vasodilation & kinetics • Decrease BP • No postural hypotension ??? • Used in Hpertension, Angina, Arrhythmia, MI, HF, Hyperthyroidism, Glaucoma & prophylaxis of Migraine headache • All cpds end with (– olol)
Propranolol (nonselective) • CVS: • Decrease CO, -ve inotropic, chronotropic, & AV & SA inhibition----- • Decrease CO, workload, & oxygen consumption--------------- • Useful in supravent. Arrhythmia but not in vent. arrhythmia • Peripheral vasoconstriction(β2, reflex response • Increase PVR ----- • Reflex vasoconst.----- • In Hypertensive patients, total PVR return to normal ore below • Gradual decreasae in syst. & diast. BP
Propranolol (cont.) • Bronchoconstriction (precipitate COPD) • Glucose metabolism (glycogenolysis, Glucagon) • Prop. + Isoproterenol • Prop + Epi ??? • Prop + NE ???
Therapeutic uses: • Hypertension (normotensive ???) • Decrease CO • Inhibit renin release from kidney • Decrease total PVR • Decrease sympathetic outflow • Angina, (chronic management of stable angina) • Myocardial infarction • Prophylactic • Immediate administration, …..? • Reduce incidence of sudden arrhythmic death after MI • Migraine (prophylactic, lipid soluble) • Hyperthyroidism
Propranolol (cont.) • Kinetics (absorption, metabolism, BBB) • Adverse effects: • Bronchoconstriction • Arrhythmia (upregulation, ppt arrhythmia) • Sexual impairment • Metabolic disturbances: • Glycogenolysis, glucagon • ppt symptoms of hypoglycemia -----? • Mobilize energy molecules ex. FFA(lipase activation, β2, β3 , bad, good cholesterol, selective β1 ) • CNS effects (CNS dep., fatigue, weakness,------, selective β1 antag.)
Drug interaction • Inhibitors: cimetidine, fluoxetine, paroxetine, and ritonavir • Inducers:barbiturates, phenytoin, and rifampin
Nadolol, Timolol: non-selective β agents • Non-selective • More potent than prop. • Nadolol: long duration • Timolol, betaxolol, carteolol------glaucoma (open-angle glaucoma, piloarpine???)
Acebutolol, Atenolol, Betaxolol, Bisoprolol, Esmolol, Metaprolol, & NebivololSelective β1 antagonists • Β1 selective, no bronchoconstriction (β2) • This occurs at doses 50 – 100 fold less than β1 • This effect disappear at high doses • So SEs are predictable • Used for hypertension & to increase exercise tolerance in angina • Esmolol given IV, short duration of action??? • Fewer effects on pulmonary system, PVR, & CHO metabolism ??? • nevibolol releases NO from endothelial SMs------? • Uses ???
Therapeutic uses: • hypertensive patients with impaired pulmonary function • first-line therapy for chronic stable angina • Bisoprolol and the extended-release formulation of metoprolol are indicated for the management of chronic heart failure • Raynaud phenomenon) is less frequent???
Acebutolol, Pindolol: antagonists with Partial Agonist Activity • Acebutolol β1 selective antagonist • Pindolol nonselective β blocker • With Intrinsic Sympathomimetic Activity (ISA)??? • Diminished effect on heart • Β blockers with ISA minimize disturbances in lipid & CHO metabolism compared with other β blockers • Effective in hypertensive patients with bradycardia
Labetalol & Carvedilol: antagonists of both α & β adrenoceptors • Labetalol, carvedilol: nonselective β-blocker with α1 blocking effect------ • Decrease BP • Carvedilol decrease lipid peroxidation, vascular wall thickening, so useful in HF • Labetalol replaced methyldopa in pregnancy hypertension & used in hypertensive crisis (IV) • SEs include orthostatic hypot. & dizziness
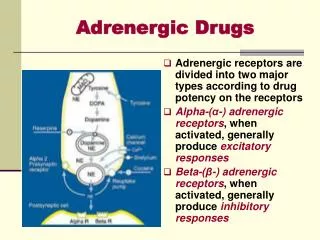
Drugs Affecting Neurotransmitter Reuptake or Release EMT: extraneuronal MAO transporter, NET: neuronal noradrenal;ine transporter
Drugs Affecting Neurotransmitter Release or Uptake Reserpine (plant alkaloid): • Blocks Mg/adenosine triphosphate (biogenic amine transporter) • Slow onset of action, long duration of action • Used in hypertension replaced with newer drugs