Download
1 / 14
140 likes | 280 Views
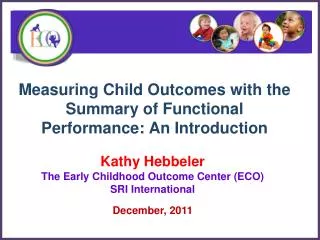
ALLHAT. ALLHAT: What Outcomes Would Have Been Expected?. Comparisons Among Placebo- or No Treatment Controlled Trials. Effect of Antihypertensive Therapy on CV Events. Fatal/nonfatal strokes. CVD deaths. Fatal/nonfatal CHD events. CHF. LVH. Percent decrease in events vs placebo.

E N D
ALLHAT ALLHAT: What Outcomes Would Have Been Expected? Comparisons Among Placebo- or No Treatment Controlled Trials
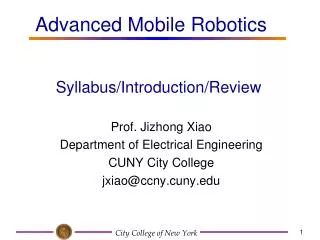
Effect of Antihypertensive Therapy on CV Events Fatal/nonfatal strokes CVD deaths Fatal/nonfatal CHD events CHF LVH Percent decrease in events vs placebo 17 randomized, placebo-controlled trials using diuretic or b-blocker (n=48,000) All reductions are statistically significant Moser M et al. J Am Coll Cardiol. 1996;27:1214-1218. Hebert PR et al. Arch Intern Med. 1993;153:578-581.
Event Reduction with “Low Dose” Diuretic or b-Blocker ns ns 25-50 mg HCTZ Psaty, et al. JAMA 1997;277:739-745
Event Reduction:SHEP & Syst-EurRandomized Controlled Trials in Isolated Systolic Hypertension (ISH) ns separately, but p<.05 combined ns ns SHEP: Systolic Hypertension in the Elderly, n=4,736; 1st drug: chlorthalidone Syst-Eur: Systolic Hypertension in Europe, n=4,695; 1st drug: nitrendipine Syst-Eur (1997) was the only randomized placebo-controlled morbidity trial in hypertension with a calcium channel blocker
HOPE Trial Effect of ACE Inhibition vs Placebo on CV Outcomes CV Death Nonfatal MI Nonfatal Stroke P < .001 New/Worsening CHF Revascularization Worsening Angina P = .001 Risk Reduction (%) Yusuf S, et al. N Engl J Med. 2000;342:145-53
Event Reduction in SHEP, Syst-Eur, and HOPE SHEP: Systolic Hypertension in the Elderly, n=4,736; chlorthalidone Syst-Eur: Systolic Hypertension in Europe, n=4,695; nitrendipine HOPE: Heart Outcomes Prevention Evaluation Study, n=9,297; ramipril
PROGRESS: Study Design Randomization (6105 patients) Eligibility (7121 patients) Study end Activetherapy Patients with a History of Cerebrovascular Disease 4mg perindopril indapamide (2.5mg*) perindopril run-in 2 mg qd 4 mg qd Placebo 2 weeks 2 weeks 4 years (open) (double-blind) (*2 mg in Japan) Neal B, MacMahon S. J Hypertens 1995;13:1869-1873
Stroke Risk Reduction in PROGRESSAll participants 28% risk reduction 0.20 0.15 0.10 0.05 0.00 95% CI 17 - 38% P<0.0001 Placebo Active: perindopril +/- indapamide Proportion with event BP difference 9/4 mm Hg (Years) 0 1 2 3 4 PROGRESS Collaborative Group. Lancet 2001;358:1033-41
Stroke and Major CVD Reduction in PROGRESS PROGRESS Collaborative Group. Lancet 2001; 358: 1033-41
ALLHAT ALLHAT: What Outcomes Would Have Been Expected? Comparisons Among Active Comparator Trials Involving Diuretic +/- Beta-Blocker (D/BB)
Large Hypertension Trials Comparing Two or More Regimens: CVD or CV Mortality Trial n BPΔ Outcomes CAPPP10,985 +3/+1 captopril not superior to D/BB NORDIL 10,881 +3/ 0 diltiazem not superior to D/BB CONVINCE 16,602 0/+1 verapamil not superior to D/BB(?equivalent?) STOP-2 6,628 0/-1 isradipine/felodipine & 0/ 0 ACEIsnot superior to D/BB INSIGHT 6,592 0/ 0 nifed GITS not superior to diuretic ANBP-2 6,083 +1/0 ACEIs not superior to diuretics ALLHAT 42,418 -3/-1 chlorthalidone superior to doxazosin, -1/+1,-2/ 0 amlodipine (HF only), lisinopril
ALLHAT ALLHAT Compared to Other Large CVD Endpoint Trials: Conclusion Findings from other major trials are totally consistent with ALLHAT’s conclusion that diuretic-based antihypertensive treatment is unsurpassed in preventing major cardiovascular morbidity and mortality, and offer some support for its superiority in reducing risk of heart failure.