Download

1 / 45
1.02k likes | 5.51k Views
Vaginal Cancer. Vaginal Cancer. Rare tumor representing only 1-2% of all gynecologic malignancies 80-90% are metastatic Mean age of patients with primary vaginal cancer is 60-65 years Most primary tumors are squamous cell in origin HPV DNA identified in VAIN. Vaginal Cancer precursors.

E N D
Vaginal Cancer • Rare tumor representing only 1-2% of all gynecologic malignancies • 80-90% are metastatic • Mean age of patients with primary vaginal cancer is 60-65 years • Most primary tumors are squamous cell in origin • HPV DNA identified in VAIN
Vaginal Cancer precursors • VAIN – avg age of VAIN 3 is 53 • Ratio of VAIN to CIN is 1:23 • 5% progress to Vaginal Ca • Hallmark of VAIN • cytologic atypia-Pleomorphisim, irreg nuclear contours and chromatin clumping • Abnormal maturation • nuclear enlargement
Vaginal Cancer precursors • VAIN 3 • usually occurs in upper third of vagina and is multifocal and diffuse in half the cases. • 1/3 of patients have a hx/o CIN • CIN coexists w/ VAIN in 10-20% of pts • Colposcopic findings are similar to those of CIN (aceto white epithelium with punctations and mosaic patterns)
Vaginal Cancer precursors VAIN 1- Proliferation of basal layer Koilocytotic atypia Enlarged pleomorphic nuclei vacuolated cytoplasm
Vaginal Cancer precursors VAIN 2- Proliferation of basal layer,crowding and loss of polarity Koilocytotic atypia Enlarged pleomorphic nuclei vacuolated cytoplasm
Vaginal Cancer precursors VAIN 3 Increased proliferation of abnormal basal and parabasal cells replacing full thickness of epithelium
Vaginal Cancer precursors • Treatment Options for VAIN • Excisional Bx for small lesions • Partial Vaginectomy • Laser Vaporization • Intravaginal 5FU cream
Vaginal Cancer: Predisposing Factors • Low socioeconomic status • History of genital warts • Vaginal discharge or irritation • Previously abnormal Pap smear • Early hysterectomy • Previous pelvic radiation (?) • In-utero exposure to DES
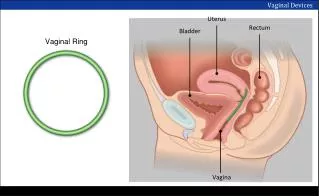
Anatomy of the Vagina • Muscular dilatable tube averaging 7.5 cm in length • Vaginal wall composed of three layers: mucosa, muscularis, adventitia. • Epithelium normally contains no glands and changes little during reproductive cycle • Lymphatic drainage of upper vagina via pelvic nodes while lower vagina drains via femoral and inguinal nodes.
Natural History and Patterns of Spread • Lesions usually found in the upper vagina on the posterior wall • Vaginal primary tumors may spread along mucosa to cervix or vulva (changes diagnosis) • Direct extension to bladder, parametria, paracolpos, rectum, cardinal ligaments, uterosacral ligaments
Gross and microscopic Findings • 50% of Vag Ca ulcerative • 30% are exophytic • 20%are annular and constricting
Natural History and Patterns of Spread • Any of the nodal groups may be involved regardless of the location of the tumor • Inguinal nodes most often involved if lesion is in the lower 1/3 of the vagina • Clinically apparent inguinal node mets seen in 5-20% of patients • Incidence of pelvic nodes varies with stage and location of the tumor
Clinical Presentation • Abnormal vaginal bleeding • 50-75% of patients with primary tumors • Dysuria • Pain
Diagnostic Work-up • Complete history and physical • Speculum examination and palpation of the vagina • Bimanual pelvic and rectovaginal examination • Pap smear, colposcopy, directed biopsies
Diagnostic Work-up • Cystoscopy • Proctosigmoidoscopy • Chest X-ray • IVP • Barium enema • Computed Tomography • MRI (84% PPV, 97% NPV)
Staging • Stage I - Lesions confined to the mucosa • Stage II- Subvaginal tissue involved but no extension to pelvic sidewall • IIA: Subvaginal infiltration only • IIB: Parametrial extension • Stage III- Pelvic sidewall extension • Stage IV- Bladder or rectal extension and/or direct extension outside of true pelvis
Natural History and Patterns of Failure • Stage I • 10-20% pelvic recurrence, 10-20% distant • Stage II • 35% pelvic recurrence, 22% distant • Stage III • 25-37% pelvic recurrence, 23% distant • Stage IV • 58% pelvic recurrence, 30% distant
Pathology • Squamous Cell CA represents 80-90% of primary tumors • Vaginal SCCA may be considered primary if there is neither cervical or vulvar CA at diagnosis or for 10 years prior • No correlation between grade and survival
Verrucous Carcinoma • Variant of well-differentiated SCCA that rarely occurs in the vagina • Relatively large, well-circumscribed, soft cauliflower-like mass • Cytologic features of malignancy are lacking • May recur locally after surgery but rarely, if ever, metastasizes
Pathology • Melanoma • 2nd most common vaginal cancer • Most frequently found in the lower third • Cells may be spindle shaped, epithelioid, or small lymphocyte-like, pigmented or non-pigmented • Junctional activity helps exclude the possibility of a metastasis • Depth of invasion best predictor of survival
Pathology • Smooth muscle tumors • Small Cell Carcinoma • Endodermal Sinus Tumor • Rhabdomyosarcoma (Sarcoma Boytrioides) • Malignant lymphoma • Clear Cell Adenocarcinoma
Management • Radiation therapy is the preferred treatment for most carcinomas of the vagina • Surgical therapy • Irradiation failures • Non-epithelial tumors • Stage I Clear cell adenocarcinomas in young women
Management • Surgery • Stage I tumors of the middle or upper third of vagina treated with radical hysterovaginectomy and PLND • Stage I tumors of the lower third of vagina which may encroach on the vulva treated with radical vulvovaginectomy and bilat. groin node dissection • Pelvic exenteration possible for more invasive lesions
Management • Stage I • Usually managed with RT • Superficial lesions (<1cm) may be treated with vaginal cylinder covering the entire vagina (6-7 Gy mucosal dose + 2-3 Gy dose to tumor) • Thicker lesions may be treated with vaginal cylinder + single plane implant • EBRT reserved for aggressive lesions (infiltrating or poorly differentiated)
Management • Stage I • Radical hysterectomy, partial vaginectomy, PLND may be used for lesions of the posterior and lateral vaginal fornices • Stage IIA • WPRT (2000cGy) + parametrial boost for 4500cGy-5,000cGy total
Management • Stage IIA • WPRT (2000cGy) + parametrial boost for 4500cGy-5,000cGy total • WPRT + combination of intracavitary and interstitial implants for 5000 to 6000 cGy total • Stage IIB, III, IVA • WPRT (4000 cGy) + parametrial boost (2500 cGy)
Management • Small Cell Carcinoma • Reasonable local control may be obtained with surgery or irradiation followed by systemic chemo • Cyclophosphamide, Adriamycin, Vincristine (CAV) X 12 cycles (some prior to initiation of RT) • Doses of RT similar to SCCA
Management • Rhabdomyosarcoma • Generally treated with a combination of surgery, RT, and chemotherapy • Vincristine, Dactinomycin, Cyclophosphamide (VAC) X 1-2 years effective adjuvant treatment for stage 1 dz • Local excision + interstitial/intracavitary RT + systemic chemo has replaced radical pelvic surgery as therapy of choice
Sarcoma Botryoides Strap cell
Management • Malignant Lymphoma • Vaginectomy and radical hysterectomy or pelvic exenteration has been used for localized vaginal tumors • Satisfactory results with pelvic RT (tele and brachytherapy) + systemic chemo • Cyclophosphamide, adriamycin, vincristine, prednisone (CHOP) X 6 cycles most often used
Clear Cell Adenocarcinoma and DES Exposure • Incidence is between 0.14 to 1.4/1000 women exposed to DES • Median age at diagnosis 19 years • Lesions found mainly in the upper 1/3 of the anterior vaginal wall • 90% of patients with early stage disease (I and II) at diagnosis
Management • Clear Cell Adenocarcinoma • Surgery for stage I lesions has advantage of ovarian preservation and better vaginal function following skin graft • Vaginectomy, radical hysterectomy PLND, paraaortic LNBx (frozen section of distal margin) • Intracavitary or transvaginal radiation can be used for small lesions • More extensive lesions: EBRT
FAVORABLE FACTORS IN SURVIVAL OF PATIENTS WITH CLEAR CELL ADENOCARCINOMA • Low stage • Older age • Tubulocystic Pattern • Small tumor diameter • Reduced depth of invasion • Negative nodal mets • Positive ho/o DES
Radiation Therapy Techniques • EBRT delivered through AP:PA portals or using 4 field “box technique” • 15 cm X 15 cm or 15 cm X 18 cm portals usually adequate • Inguinal nodes should be electively covered (4500-5000cGy) for tumors of the lower 1/3 of vagina • Additional 1500cGy (4-5cm depth) delivered for palpable inguinal nodes
Radiation Therapy Techniques Portal for pelvic RT and elective groin coverage Portal for groin coverage with palpable inguinal nodes
Radiation Therapy Techniques • Intracavitary therapy utilizes vaginal cylinders (Burnett, Bleodorn, Delclos, or MIRALVA applicators) • Upper 1/3 lesions can be treated with tandem and ovoids • Interstitial therapy with 137Cs, 226Ra, or 192Ir needles have been used • High dose rate brachytherapy (>1200cGy/hour) also used
Summary • Superficial stage I lesions may be treated with RT or radical hysterovaginectomy • Stage IIA-IVA treated with WPRT and intracavitary RT • Role of chemotherapy in advanced SCCA presently unknown • Pelvic failures and distant metastases occur in 1/2 of pts with advanced dz