Download
1 / 13
170 likes | 877 Views
Polyuria-polydipsia. Central diabetes insipidus Nephrogenic diabetes insipidus Psychogenic water drinking Diabetes mellitus. Survey of diabetes insipidus. History quantitation of daily fluid intake and output noturia or enuresis detailed dietary history

E N D
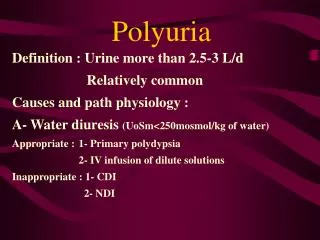
Polyuria-polydipsia • Central diabetes insipidus • Nephrogenic diabetes insipidus • Psychogenic water drinking • Diabetes mellitus
Survey of diabetes insipidus • History • quantitation of daily fluid intake and output • noturia or enuresis • detailed dietary history • avoid foods with a high protein content • acuteness of onset • drug • growth and development
Survey of diabetes insipidus • Lab • 24h I/O • Urine: specific gravity or osmo., glucose • Serum sodium and osmo. • definite diagnosis: water deprivation test
Water deprivation test • Prcedure • morning: empty bladder & weigh pt • NPO • blood: Na, K, Ca, Crea, osmo., vasopressin • q1h check: • BW • Urine: vol. , specific gravity(sg), osmolality • Serum: Na, osmolality
Water deprivation test • Ending (one of following) • BW > 3% • serum Na > 150mmol/L or osmo. > 300 mmol/L • Uosmo reaches 850 mmol/kg for 2 consecutive tests • Uosmo stablized ( < 30mmol/kg between the last 2 collections) • Empty bladder • Blood: osmo., Na, and vasopressin • DDAVP (2ug) s.c. or 10ug (0.1 ml) intranasal, and drink as desired • Uosmo and Sosmo q30min x 2, (x4 if intranasal)
Interpretation • Normal response • Uosmo to 500 – 1400 mosm/kg • U/O decrease • Sosmo: in normal range (< 295 mmol/kg) • U/P ratio > 2 • ADH: no increase in Uosmo and no decreased U/O • DI • Uosmo: no increase, U/O: no decrease • Sosmo increases (U/S ration < 2) • ADH: CDI: U/O decrease, Uosmo increase NDI: no response
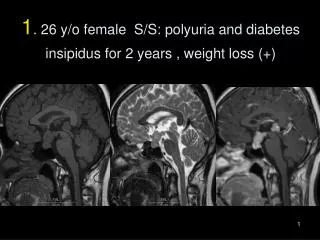
Central diabetes insipidus • Cause • brain tumor • idiopathic • neurosurgery • head trauma • HIE • histiocytosis • Survey: skull x-ray or head CT • Tx: hormonal replacement
Nephrogenic diabetes insipidus • Cause • congenital • acquired: chronic renal Dz • e- disorder: hypokalemia, hypercalcemia • sickle cell trait • adrenal insufficiency • drug • lithiium, colchicine, constrast, diuretics • diet • protein starvation, chronic salt depletion, chronic high water intake
Nephrogenic diabetes insipidus • Survey • electrolyte • renal echo • Treatment • low sodium diet (< 1mmol/kg/24h) • adequate protein (2g/kg/day) • 300-400 ml/kg water • drug: • thiazide (hydrochlorothiazide 2-4mg/kg/d):注意hypokalemia, 可與 amiloride併用 • indocin (2mg/kg/d):亦可與 thiazide併用
Water deprivation test • Prcedure • morning: empty bladder & weigh pt • NPO • blood: Na, K, Ca, Crea, osmo., vasopressin • q1h check: • BW • Urine: vol. , specific gravity(sg), osmolality • Serum: Na, osmolality
Water deprivation test • Ending (one of following) • BW > 5% (or 3%) • serum Na > 150mmol/L and plasma osmo. > 305 mmol/kg • Uosmo reaches 850 mmol/kg for 2 consecutive tests • Uosmo stablized ( < 30mmol/kg between the last 2 collections) • Empty bladder • Blood: osmo., Na, and vasopressin • DDAVP (2ug) use, and drink as desired • Uosmo and Sosmo q30min x 2