Download
1 / 6
60 likes | 191 Views
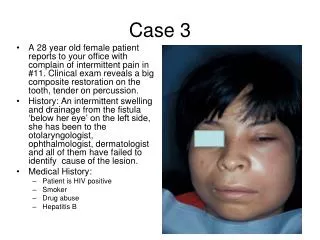
CASE 3. Dr Amit Dinda, AIIMS, New Delhi. A 51-year-old non- diabetic male presented with easy fatiguability and dyspnoea on exertion for three months. On examination he was found to be hypertensive (blood pressure 150/90 mmHg). He had pallor and mild icterus.

E N D
CASE 3 Dr Amit Dinda, AIIMS, New Delhi
A 51-year-old non- diabetic male presented with easy fatiguability and dyspnoea on exertion for three months. • On examination he was found to be hypertensive (blood pressure 150/90 mmHg). He had pallor and mild icterus. • Rest of the general physical and systemic examination was within normal limits.
Investigations • Hemoglobin - 6.8 g/dl, • Total leukocyte count of 4800/mm3, • Platelet count of 120,000/mm3 with reticulocytosis (6%). • Blood urea (80 mg/dl) and serum creatinine (3.0 mg/dl) were elevated. • 24 hour urine albumin was 0.68gm. • Serum haptoglobin levels were low (6.0 mg/dl). Liver function tests showed mild unconjugated hyperbilirubinemia (indirect bilirubin 2.0 mg/dl). • He also had elevated ldh levels (2965 iu/l)
Ultrasonographic examination showed normal sized kidneys with normal echo texture and maintained corticomedullary differentiation. Magnetic Resonance Imaging (MRI) showed reversal of normal MRI image of the kidney with hyper intense renal cortex compared to the medulla and persistence of lowered signal intensity in T2 weighted images (Fig.1). • In view of unexplained renal failure he underwent a kidney biopsy. A representative photomicrograph of the biopsy is provided (Fig.2)