Download
1 / 62
760 likes | 1.75k Views
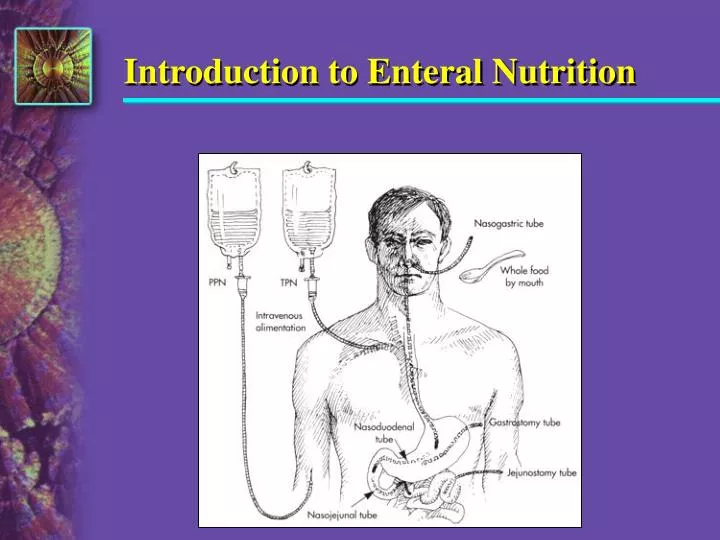
Introduction to Enteral Nutrition. Enteral Nutrition. Nutrition delivered via the gut Includes oral feedings and tube feedings. Enteral Tube Feeding. Nutritional support via tube placement through the nose, esophagus, stomach, or intestines (duodenum or jejunum)

E N D
Enteral Nutrition • Nutrition delivered via the gut • Includes oral feedings and tube feedings
Enteral Tube Feeding • Nutritional support via tube placement through the nose, esophagus, stomach, or intestines (duodenum or jejunum) —Must have functioning GI tract —IF THE GUT WORKS, USE IT! —Exhaust all oral diet methods first.
Oral Supplements • Between meals • Added to foods • Added into liquids for medication pass by nursing • Enhances otherwise poor intake • May be needed by children or teens to support growth
Diagram of enteral tube placement. Fig. 22-2. p. 468.
Conditions That Require SpecializedNutrition Support • Enteral —Impaired ingestion —Inability to consume adequate nutrition orally —Impaired digestion, absorption, metabolism —Severe wasting or depressed growth • Parenteral —Gastrointestinal incompetency —Hypermetabolic state with poor enteral tolerance or accessibility
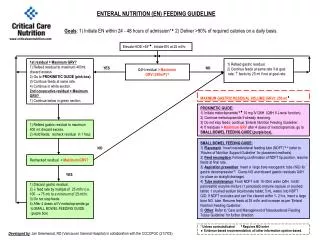
Algorithm for Decisions Modified and adapted from Gorman RC, Morris JB: Minimally invasive access to the gastrointestinal tract. In Rombeau JL, Rolandelli RH, editors: Clinical nutrition: enteral and tube feeding, p 174, Philadelphia, 1997, WB Saunders; and Ali A et al: Nutritional support services, Nutritional Support Algorithms, 8(7):13, July 1998.
Indications for Enteral Nutrition • Malnourished patient expected to be unable to eat >5-7 days • Normally nourished patient expected to be unable to eat >7-9 days • Adaptive phase of short bowel syndrome • Increased needs that cannot be met through oral intake (burns, trauma) • Inadequate oral intake resulting in deterioration of nutritional status or delayed recovery from illness ASPEN. The science and practice of nutrition support. A case-Based Core curriculum. 2001; 143
Contraindications for EN • Severe acute pancreatitis • High output proximal fistula • Inability to gain access • Intractable vomiting or diarrhea • Aggressive therapy not warranted ASPEN. The science and practice of nutrition support. A case-based core curriculum. 2001; 143
Contraindications for EN • Inadequate resuscitation or hypotension; hemodynamic instability • Ileus • Intestinal obstruction • Severe G.I. Bleed • Expected need less than 5-7 days if malnourished or 7-9 days if normally nourished
Advantages - Enteral vs PN • Preserves gut integrity • Possibly decreases bacterial translocation • Preserves immunological function of gut • Reduces costs (EAL Grade II) • Fewer infectious complications in critically ill patients (EAL Grade I) • Safer and more cost effective in many settings ASPEN. The science and practice of nutrition support. A case-based core curriculum. 2001; 147 ADA EAL, Critical Illness, accessed 8-07
Advantages—Enteral Nutrition • Intake easily/accurately monitored • Provides nutrition when oral is not possible or adequate • Supplies readily available • Reduces risks associated with disease state
Disadvantages—Enteral Nutrition • GI, metabolic, and mechanical complications—tube migration; increased risk of bacterial contamination; tube obstruction; pneumothorax • Costs more than oral diets (not necessarily) • Less “palatable/normal”: patient/family resistance • Labor-intensive assessment, administration, tube patency and site care, monitoring
Enteral Formulas • Liquid diets intended for oral use or for tube feeding • Ready-to-use or powdered form • Designed to meet variety of medical and nutrition needs • Can be used alone or given with foods
Formula Selection • Functional status of GI tract • Physical characteristics of formula (osmolality, fiber content, caloric density, viscosity) • Macronutrient ratios • Digestion and absorption capability of patient • Specific metabolic needs • Contribution of the feeding to fluid and electrolyte needs or restriction • Cost effectiveness The suitability of a feeding formula should be evaluated based on
Enteral Formulas • Determine best choice by medical and nutrition assessment • Meet specific nutrition needs
Enteral Formulas • Complete formulas: • Enteral formulas designed to supply all needed nutrients when given in sufficient volume • May also be used in smaller quantities to supplement regular diets
Enteral Formula Categories • Polymeric • Monomeric • Fiber-containing • Disease-specific • Rehydration • Modular
Enteral Formula CategoriesPolymeric • Whole protein nitrogen source • For use in patients with normal or near normal GI function • Protein isolate formulas • Protein that has been separated from a food (casein from milk, albumin from egg) • Blenderized formulas • May contain pureed meat, vegetables, fruits, milk, starches with v/m added • Made at home or purchased commercially
Enteral Formula CategoriesMonomeric • Elemental/hydrolyzed • Predigested nutrients • Free amino acids and/or short peptide chains • Has low fat content or high percentage of MCT, LCT, structured lipids
Enteral Formula CategoriesMonomeric • Use in patients with compromised digestive and/or absorptive capacity • More expensive than standard formulas • Tend to be more hyperosmolar because of small particle size
Enteral Formula CategoriesFiber-Containing • Fiber-containing: containing a source of fiber; reportedly beneficial for prevention/treatment of altered bowel function in enterally fed patients • Soy polysaccharide is the most common fiber additive in enteral feedings; effectiveness in treating diarrhea in tubefed patients unproven ASPEN. The science and practice of nutrition support. A case-based core curriculum. 2001; 148
Enteral Formula CategoriesFiber-Containing • Soluble fiber (guar gum, oat fiber, pectin) may exert trophic effect on colonic mucosa and be useful in normalizing bowel function • Most enteral feedings in amounts typically used contain less than recommended fiber intake for adults (20-35 g) • Patients with impaired gastric emptying should not be fed fiber-containing formula into the stomach ASPEN. The science and practice of nutrition support. A case-based core curriculum. 2001; 148
Enteral Formulas: Calorie Dense • May be used in fluid-restricted or volume-sensitive patients • Useful for nocturnal feedings where nutrition must be delivered over brief time span • Calorie density ranges from 1.3 to 2 kcals/ml • Monitor fluid/hydration status
Enteral Formula CategoriesDisease Specific • Designed for patients with specific disease states. • Available for patients with respiratory disease, ARDS, diabetes, renal failure, hepatic failure, and immune compromise. • Well-designed clinical trials may or may not be available (mostly not) • Many of the trials have been done with formula “cocktails,” making it difficult to identify the operative variable
Enteral Formula CategoriesDisease Specific • Pharmaceutical effects are claimed for many specialty enteral formulas (reduced LOS, reduced infections, reduced time on the ventilator) • Mfrs are charging pharmaceutical prices (8-10 times more expensive than standard) • Enteral formulas are classed as medical foods, not drugs and are regulated differently
Enteral Formula CategoriesDisease Specific • The FDA does not evaluate adult medical foods before they go on the market • The government does not require that mfrs prove that formulas are safe and effective or that claims are valid • FDA requires that formula mfrs use good manufacturing practices and that products are accurately labeled • It is up to the clinician to evaluate the evidence that supports the claims regarding medical foods
Considerations in Evaluating Specialized Enteral Formulas • Is the nutrient profile appropriate based on the known metabolic needs and nutrient requirements of the condition • Are there prospective double-blind RCTs to support claims (not case reports) • Data obtained using animal models may have limited application to humans • Product-specific research applies to that product only
Enteral FormulasEvaluating the Research • Research cannot always be generalized to a different population (studies in burn patients to trauma pts) • Were the endpoints clinically significant (a biochemical marker only or important clinical outcome such as wound healing)? • Who funded the study? • Has the work been replicated?
Disease Specific FormulasDiabetic • Amount and type of CHO modified to reduce blood glucose response • Increased fat content (may have increased monounsaturated fats) • Results of studies using these formulas have been mixed • Most standard enteral formulas fall within American Diabetes Association guidelines for macronutrient mix
Disease Specific FormulasDiabetic • Blood glucose control in acute care is often affected by illness, infection, other issues • Patients on enteral feedings generally receive a more consistent CHO intake than persons on oral diets • May be worth trying diabetes formulas in patients who have failed to achieve good blood glucose control on standard formulas
Disease Specific FormulasHepatic • Generally have reduced aromatic amino acids and increased branched chain amino acids • More expensive than standard products • Often lower in protein than standard formulas (may be too low for most liver patients) • Research using these products has been inconclusive • Standard (high protein) products are generally appropriate for patients with liver disease
Disease Specific FormulasRenal • Originally developed in an effort to delay the need for dialysis as long as possible • Typically are calorie dense (2.0 kcal/cc) products with relatively low protein levels and modified electrolytes • Generally too low in protein for dialyzed patients and acutely ill patients • May be useful for short term use as supplement or calorie source in pre-dialysis chronic renal failure patients
Disease-Specific Formulas Renal Novasource Renal
Disease Specific FormulasImmune-Enhancing • Have added “immune-enhancing” nutrients (arginine, glutamine, omega-3 fatty acids, nucleotides) • Results of research have been mixed • Multiplicity of active ingredients makes it difficult to control variables • Meta-analysis suggests that they might be most beneficial in surgical patients • Some evidence of harm in septic patients
Immune-Enhancing EN in Critical Care: ADA Evidence-Based Guidelines • R.3 Immune-enhancing EN is not recommended for routine use in critically ill patients in the ICU. • Immune-enhancing EN is not associated with reduced infectious complications, LOS, reduced cost of medical care, days on mechanical ventilation or mortality in moderately to less severely ill ICU patients. • Their use may be associated with increased mortality in severely ill ICU patients, although adequately-powered trials evaluating this have not been conducted. • Strength: Fair; imperative
Immune-Enhancing EN in Critical Care: ADA Evidence-Based Guidelines • For the trauma patient, it is not recommended to routinely use immune-enhancing EN, as its use is not associated with reduced mortality, reduced LOS, reduced infectious complications or fewer days on mechanical ventilation. Source: ADA EAL Evidence-Based Guidelines, accessed 8/07
Disease-Specific FormulaPulmonary • Contain higher percentage of total calories from fat to reduce respiratory quotient and make it easier to wean from respirator • However, total calorie intake has more impact on respiratory function than formula composition • There is a lack of clinical trials demonstrating a clear benefit • High fat gastric feedings may cause delayed emptying in critically ill patients
Enteral Formula CategoriesRehydration and Modular • Rehydration: for patients requiring optimal ratio of carbohydrate to electrolytes to facilitate fluid and electrolyte absorption, rehydration • Modular: provides protein, fat, or carbohydrate as single nutrients or modular mixtures to allow adjustment of macronutrient mix. May also contribute to renal solute load, osmolality
Enteral Formula Nutrient SourcesCarbohydrate • CHO content ranges from 40-90% of total calories • Typically some combination of hydrolyzed cornstarch, maltodextrins, corn syrup solids, sucrose • FOS: fructooligosaccharides; poorly absorbed in the small intestine, fermented in the large intestine; may promote growth of healthy bacteria • Fiber: soy polysaccharide (most common) guar gum, oat fiber, pectin
Enteral Formula Nutrient SourcesLipids • Fat provides isotonic, concentrated energy source • Corn and soybean oil common • Also safflower, canola, fish oil • May include MCTs; more easily digested and absorbed • Fat content ranges from <10% to >50% of calories ASPEN. The science and practice of nutrition support. A case-based core curriculum. 2001; 148