Download
1 / 23
270 likes | 593 Views
Diarrhea in ICU setting. B89401129 楊展輝. Patient. 蘇 xx 娥 4226891 72 y/o Female ER 10/16 4:46pm acute onset chest pain radiating to back + cold sweating since that afternoon 4pm T/P/R 35.9/96/24 BP 194/80mmHg Rectal CA s/p OP, C/T and cholecystectomy at 和信 H. 10+ yrs ago

E N D
Diarrhea in ICU setting B89401129 楊展輝
Patient • 蘇xx娥 4226891 • 72 y/o • Female • ER 10/16 4:46pm • acute onset chest pain radiating to back + cold sweating since that afternoon 4pm • T/P/R 35.9/96/24 BP 194/80mmHg • Rectal CA s/p OP, C/T and cholecystectomy at和信H. 10+ yrs ago • HTN 20+ yrs without regular control • DM 3 yrs under OHA
Dissecting aortic aneursym arising from aortic root and extension almost down to the aortic bifurcation. Calcified intimal flap. The celiac trunk, SMA and left renal artery arise from the true lumen, but the right renal artery arise from the false lumen. Cardiomegaly.
Dx: Debakey type I DAA with moderate AR s/p aortic grafting with 24mm Hemashield and epicardial pacemaker Dacron graft • Post-OP -> ICU 10/17 • Sternum dehiscence s/p debridement and sternum closure on 10/25 • Sternum dehiscence s/p debridement and unapproximated sternum (osteoporosis) on 10/31
10/31, 11/20 B/C: MRSA • 10/31, 11/22 sternal wound culture: MRSA • Vancomycin 10/31~11/23, Zyvox 11/23~ • Sternal wound MRSA infection with mediastinitis s/p RA & bilateral PM rotational flap + STSG on 11/6 • 11/16 S/C: K.p (3+). 11/29, 12/2 S/C: Enterobacter cloacae • CMZ 11/16~11/18, Fortum 11/19~11/29. • Invanz 12/1~12/11 • Extubation on 12/6 -> O2 mask
Abrupt onset, intermittent, 11/15~ (>4 wks), no travel, yellow, watery, no abdominal pain • 11/19, 12/6 Stool: no Clostridium difficile • 12/6 Stool: Candida tropicalis 3+ • 12/8 Surgical wound x II: Candida albicans • 12/12 Colonoscopy: internal hemorrhoids, s/p OP • 12/14 Clostridium difficile toxin A (-)
Factors Contributing to Diarrhea? • Medication: • Gaster 1# BID 10/20~ • Histamine H2 Antagonist • Serious Adverse Effectsa) Increased liver enzymesb) Necrotizing enterocolitis in fetus OR newborn • Paramol 1# QID 11/9~12/13 • Serious Adverse Effectsa) Gastrointestinal hemorrhageb) Hepatotoxicityc) Nephrotoxicityd) Pneumonitis • Enteral diet: • Nu-pep (100% peptide, 8% medium TG) • Alitraq (27% Glutamine, peptide & free a.a., 53% medium TG)
290 - 2 x (Na +K)> 125 Candida tropicalis 3+
Harrison's Internal Medicine > Part 4. Nutrition • Enteral feeding often causes diarrhea, especially if bowel function is compromised by disease or drugs, particularly broadspectrum antibiotics. Diarrhea may be controlled by the use of a continuous drip, with a fiber-containing formula or by adding an anticholinergic medication to the formula. Diarrhea associated with enteral feeding does not necessarily imply inadequate absorption of nutrients, other than water and electrolytes. Since luminal nutrients exert trophic effects on the gut mucosa and enhance the enteric immunologic barrier, it is often appropriate to persist with tube feeding, despite the diarrhea, even when this necessitates supplemental parenteral fluid support.
Flagyl 11/30~12/2, 12/10~12/14 • Mycostatin 12/12~12/18 • Invanz 12/1~12/11 • Zyvox 11/23~
Role of candida in pathogenesis of antibiotic-associated diarrhea in elderly patients • 24 elderly inpatients (mean age 74 years) • negative for Clostridium difficile toxin • 7 had intestinal overgrowth of Candida species (>/= 10e5 cfu/ml) • None abx treated controls without diarrhea had candida overgrowth • 5/7 -> nystatin -> resolution of diarrhoea, candida <10e4 cfu/ml in 7 days (still on abx) • 2/7 diarrhoea subsided spontaneously and candida turned normal (<10e4 cfu/ml) after abx withdrawn. Lancet 1991; 337: 511-14.
Chromagar: 1) C. albicans, 2) C. glabrata, 3) C. tropicalis, 4) C. krusei edoc.hu-berlin.de
Clostridium difficile consistently associated with nosocomial diarrhoea • C difficile toxin positive 35-40%, cause unknown 60-65%. • Abx >> bacterial supression >> candida overgrowth >> bacterial supression >> diarrhea • No leukocytes found, so not an intestinal invasive disease • No evidence of colitis in colonoscopy • Secretory in nature, etiology? Lancet 1991; 337: 511-14.
Mechanisms and Management of Antibiotic-Associated Diarrhea • Diarrhea is a frequent adverse effect of antibiotics • Diarrhea: mushy or watery stool >200g/day or >3 times/day • Candida toxin: secreted aspartyl proteinases (Saps) and phospholipases • Anaerobs: carbohydrate -> SCFAs (fluid/electrolytes absorption & energy for distal colon mucosa) Clinical Infectious Diseases 1998;27:702–10
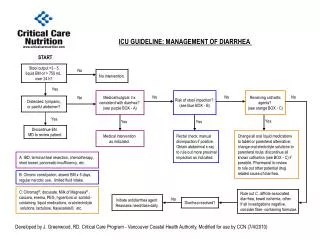
Treatment • Withdraw Abx unless indication correct • Change Abx to less CDAD (quinolones, sulfonamides, iv amnioglycosides, co-trimoxazole, metronidazole, tetracycline) • Probiotics: Saccharomyces boulardii & Lactobacillus • Nystatin (0.25~1MU TID~QID) • Substitute lost fluid & electrolytes • Avoid poor absorbable dietary carbohydrates Clinical Infectious Diseases 1998;27:702–10