Download
1 / 1
10 likes | 120 Views
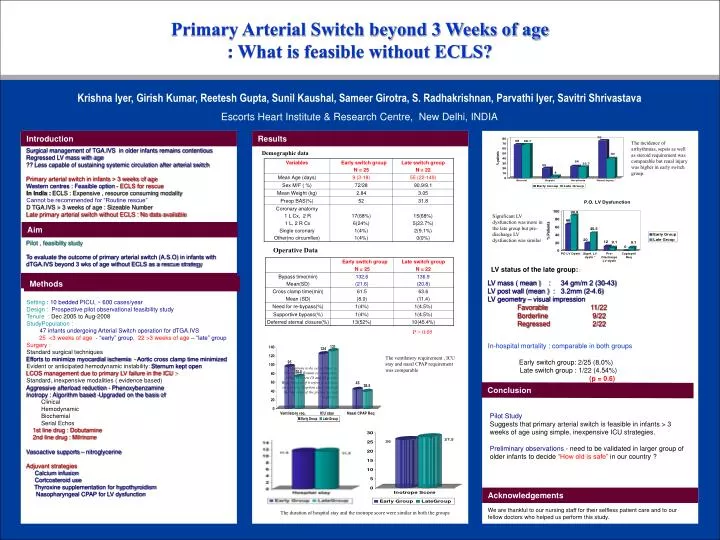
Primary Arterial Switch beyond 3 Weeks of age : What is feasible without ECLS?. Krishna Iyer, Girish Kumar, Reetesh Gupta, Sunil Kaushal, Sameer Girotra, S. Radhakrishnan, Parvathi Iyer, Savitri Shrivastava Escorts Heart Institute & Research Centre, New Delhi, INDIA.

E N D
Primary Arterial Switch beyond 3 Weeks of age : What is feasible without ECLS? Krishna Iyer, Girish Kumar, Reetesh Gupta, Sunil Kaushal, Sameer Girotra, S. Radhakrishnan, Parvathi Iyer, Savitri Shrivastava Escorts Heart Institute & Research Centre, New Delhi, INDIA LV mass ( mean ) : 34 gm/m 2 (30-43) LV post wall (mean ) : 3.2mm (2-4.6) LV geometry – visual impression Favorable 11/22 Borderline 9/22 Regressed 2/22 In-hospital mortality : comparable in both groups Early switch group: 2/25 (8.0%) Late switch group : 1/22 (4.54%) (p = 0.6) Introduction Results The incidence of arrhythmias, sepsis as well as steroid requirement was comparable but renal injury was higher in early switch group. Surgical management of TGA.IVS in older infants remains contentious Regressed LV mass with age ?? Less capable of sustaining systemic circulation after arterial switch Primary arterial switch in infants > 3 weeks of age Western centres : Feasible option - ECLS for rescueIn India : ECLS : Expensive , resource consuming modality Cannot be recommended for “Routine rescue” D TGA.IVS > 3 weeks of age : Sizeable Number Late primary arterial switch without ECLS : No data available Demographic data Significant LV dysfunction was more in the late group but pre-discharge LV dysfunction was similar Aim Pilot , feasibilty study To evaluate the outcome of primary arterial switch (A.S.O) in infants with dTGA.IVS beyond 3 wks of age without ECLS as a rescue strategy Operative Data LV status of the late group: : Methods Methods Setting : 10 bedded PICU, ~ 600 cases/year Design : Prospective pilot observational feasibility study Tenure : Dec 2005 to Aug-2008 StudyPopulation : 47 infants undergoing Arterial Switch operation for dTGA.IVS 25 <3 weeks of age - “early” group, 22 >3 weeks of age – “late” group Surgery : Standard surgical techniques Efforts to minimize myocardial ischemia - Aortic cross clamp time minimized Evident or anticipated hemodynamic instability: Sternum kept open LCOS management due to primary LV failure in the ICU :- Standard, inexpensive modalities ( evidence based) Aggressive afterload reduction - Phenoxybenzamine Inotropy : Algorithm based -Upgraded on the basis of Clinical Hemodynamic Biochemial Serial Echos 1st line drug : Dobutamine 2nd line drug : Milrinone Vasoactive supports – nitroglycerine Adjuvant strategies Calcium infusion Cortcosteroid use Thyroxine supplementation for hypothyroidism Nasopharyngeal CPAP for LV dysfunction P > 0.05 The ventilatory requirement , ICU stay and nasal CPAP requirement was comparable Captions to be set in Times or Times New Roman or equivalent, italic, between 18 and 24 points. Right aligned if it refers to a figure on its right. Caption starts right at the top edge of the picture (graph or photo). Conclusion Pilot Study Suggests that primary arterial switch is feasible in infants > 3 weeks of age using simple, inexpensive ICU strategies. Preliminary observations- need to be validated in larger group of older infants to decide “How old is safe” in our country ? Acknowledgements We are thankful to our nursing staff for their selfless patient care and to our fellow doctors who helped us perform this study. The duration of hospital stay and the inotrope score were similar in both the groups