Download
1 / 20
200 likes | 289 Views
Explanations for the Decline in Health Insurance Coverage. Michael Chernew, Michigan and NBER David Cutler, Harvard and NBER Patricia Keenan, Harvard.

E N D
Explanations for the Decline in Health Insurance Coverage Michael Chernew, Michigan and NBER David Cutler, Harvard and NBER Patricia Keenan, Harvard This work was funded by the Economic Research Initiative on the Uninsured, the National Institutes on Aging, and the Alfred P. Sloan Foundation.
Research Questions • What impact will rising premiums have on coverage in the future? • What role did rising premiums for health insurance play in declining coverage rates over the 1990s?
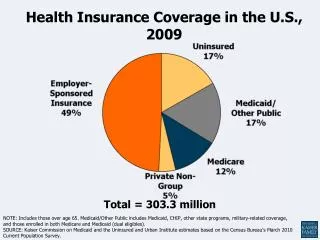
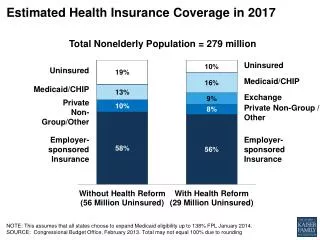
Basic Fact • Despite strong economic growth, and expanding public coverage, the rate of health insurance coverage fell during the 1990s. • 13.7% of non-elderly uninsured (1987) • 15.8% of non-elderly uninsured (2000)
Reasons for Decline • Demographic or labor market changes • Changing value of alternatives (charity care) • Equilibrium unraveling • Increase in working spouses • Regulatory changes • Changing Load • Taxes • Rising premiums • 1% increase in premium drop of 300,000 (Lewin)
‘Load’ as a Measure of Price • Textbook models: • ‘Price’ is the load (difference between premium and expected payout) • Rising premiums • Have no ‘price’ effect • May lead to greater coverage if correspond to greater risk • Most elasticity estimates are ‘load’ or ‘co-premium based’
Why Premiums May Matter • Higher premiums may include greater moral hazard cost • Contracting imperfect • Higher premiums may increase incentives for low risk to opt out and market to unravel • Higher premiums may increase relative appeal of charity care • Particularly if better technology (which drives up premiums) is also partially available via charity care
Control for: Individual traits Taxes Working spouses Medicaid expansion Immigration State insurance regulation MSA unemployment MSA demographics Managed care enrollment Approach • Relate decline in coverage between 1988-1990 and 1998-2000 to increases in premiums • Probit model using individual level data
Individual Data • Insurance Coverage • Demographics and employment characteristics for individuals and family head • Time interactions • Income deciles (Gruber approach) • Income deciles interacted with marital status of family head • Income deciles interacted with marital status and time • Child age dummies, mean medical care spending by child age (Cutler /Gruber 1996).
BaseResultsAny Cov. Private Public Controls for individual level traits and MSA demographics included but not displayed.
Endogeneity and Attenuation bias • Noise in premium measure • Uninsured may cause rising costs • Selection effects • Cost shifting • Instrument with Medicare and State per capita costs • F-stat: 52.66 • Partial R-squared: .75
BaseResults - IV Any Cov. Any Cov. Any Cov. Probit LPM LPM - IV Instruments for private premiums are Medicare Part B and state nonelderly medical spending. Controls for individual level traits and MSA demographics included but not displayed.
Premium Results by SubgroupAny Cov. Private Public Controls for all covariates in base model.
Interpretation • 1% increase in premiums leads to 150,000 more uninsured • Half of Lewin effect • 1% cost growth above GDP leads to 1.8M more uninsured • 2% cost growth above GDP leads to 3.8M more uninsured • Mean premium increase ($645) accounts for: • 1.7 percentage points decline in coverage • ~54% of mean decline • Effects greatest for young and low income
Conclusions • Health care cost increases are related to drop in coverage. • It is reasonable to assume that coverage rates will continue the long-term decline. • Subsidy and pro-competition strategies may be short term fixes • Suggests a fundamental challenge to policy makers • Individuals desire access to new medical technologies • Costs of coverage may become increasingly less affordable
Explaining Tax Results • Results are not robust to specification changes • Very little variation in taxes rates over time • Fixed effects absorb much of this variation • Counter-intuitive results likely noise • We don’t focus on groups most likely to be affected • Private coverage • Workers • Workers own employment-based coverage results are consistent with literature
Sensitivity of ‘Any Coverage’ to Cost Measure Private premiums Medicare Pt. B Controls for individual level traits and MSA demographics included but not displayed.
Other findings • Medicaid expansions increase coverage 1 percentage point • Some variables reduce private, but not public, coverage • Working women • Premiums • Demographic forces offset • Income vs. other demographics
Focus on ‘Any Coverage’ • Advantage • Broadest measure of coverage trends • Disadvantage • Effects may differ in sub-markets • Private • Workers • Own ESI • Public
Model • Coverage i,m,t = X i,m,t Bt + Zm,tl + dm+ qt + e i,m,t • Standard errors assume clustering by MSA*time