Download
1 / 48
500 likes | 931 Views
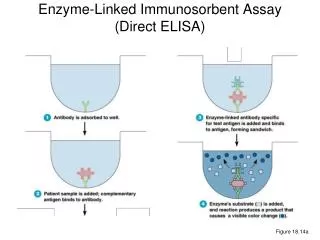
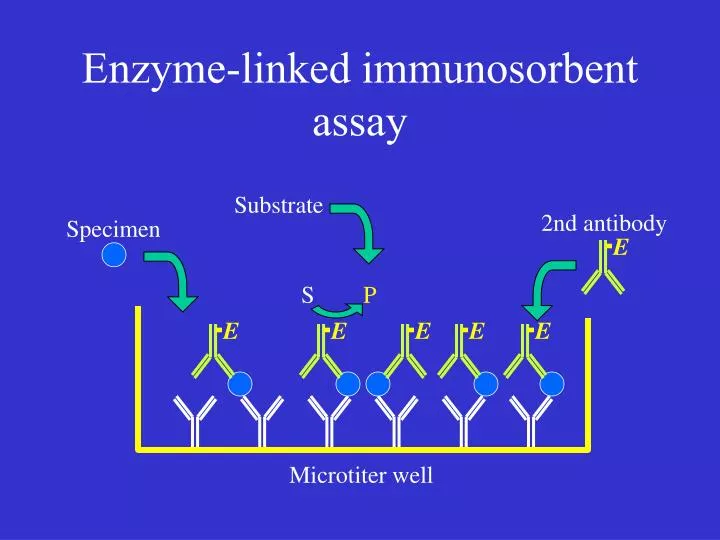
Substrate. E. E. E. E. E. E. 2nd antibody. Specimen. S. P. Microtiter well. Enzyme-linked immunosorbent assay. Substrate. E. E. E. E. E. 2nd antibody. S. P. HAMA “bridging” interference. E. E. E. E. HAMA blocking interference.

E N D
Substrate E E E E E E 2nd antibody Specimen S P Microtiter well Enzyme-linked immunosorbent assay
Substrate E E E E E 2nd antibody S P HAMA “bridging” interference
E E E E HAMA blocking interference
Distinguishing between Health and Disease: The role of the clinical laboratory in the diagnostic process Clinical Biochemistry 3H3
What is normal??? • Normal Health • choice between defining an ‘ideal state’ or determining an ‘average’ state in people considered healthy • more practical to analyze ‘average’ state --with respect to a biological parameter results in a symmetric (Gaussian) distribution
The Disease State • A population having a specific disease will usually have an asymmetric (nonparametric) distribution.
Diagnostic process involves gathering information until, ideally, the probability of the disease approaches 100%. in practice, this value is much lower at the time of the decision.
Defining the value of a Diagnostic Test • The clinical performance of a laboratory test defines how well it predicts disease • The sensitivity of a test indicates the likelihood that it will be positive when disease is present • The specificity of a test indicates the likelihood that it will be negative when disease is absent • Distinction between a test being a true positive (TP) or true negative (TN) is usually determined with reference to a selected “normal range” based on 95% confidence. This range is referred to as a Reference Range (RR). Test focuses on the upper or lower limit often use a Reference Value (RV). • False Positive (FP) Normal people falling outside RR • False Negative (FN) Diseased individual falling inside RR
Defining the value of a Diagnostic Test • Reference state (RS): conditions in which the RR is assumed to apply • “Ideal world” RS would include sex, ethnicity, weight range, diet • In practice RR are applied to a much larger population • distinction made between neonate, pediatric, obstetrics and geriatric practices • Establishing a Reference Range • min 100 subjects • Test should be validated under the following conditions: • in healthy subjects • in patients with the disease • no symptoms • full symptoms • subjects who not have the disease but whose signs and symptoms mimic the disease • subjects having a pathologic conditions associated with the same organ system
Laboratory Test Characteristics • Sensitivity(SENS)- the test “positivity” SENS= TP X 100 TP +FN =% of disease cases that give a positive result with the RV selected • Specificity(SPEC)- the test “negativity” SPEC= TN X 100 TN +FP =% of non-disease cases that give a negative result with the RV selected
Example Of 25 admitted cocaine abusers, 23 tested positive for urinary benzoylecgonine and 2 tested negative. What is the sensitivity of the urine screen?
Sensitivity and specificity are inversely related. Marker concentration - + Disease
Do you prefer a sensitive test or a specific test? • Choice of test characteristic is a function of diagnostic need • Discovery tests are often applied to asymptomatic patients. • requires good sensitivity • Confirmatory tests require high specificity • establish presence of disease • Test to exclude a disease require high sensitivity • little chance of false negatives
Evaluating Clinical Performance of laboratory tests • The sensitivity of a test indicates the likelihood that it will be positive when disease is present • The specificity of a test indicates the likelihood that it will be negative when disease is absent • The predictive value of a test indicates the probability that the test result correctly classifies a patient
Laboratory Test Characteristics(Cont) • Prevalence of a disease is the number of positive cases in the population being tested at a designated point in time. • 1 per X people, number per 100, 000, or expressed as percentage • Predictive Value (PV)- essential characteristic of any lab test. Depends on: SENS, SPEC and prevalence • indicates info that can be gained from by conducting test under a giving set of conditions PV(+) = TP X 100 TP +FP PV(-) = TN X 100 TN +FN
Predictive Value The predictive value of a clinical laboratory test takes into account the prevalence of a certain disease, to quantify the probability that a positive test is associated with the disease (PV+) in a randomly-selected individual, or alternatively, that a negative test is associated with health (PV-).
Laboratory Test Characteristics SPEC= TN X 100 TN +FP 88 X 100= 88% 88 +12 New test devoloped for Myocardial infarction (cTnI) 35% prevalence of MI Research Data 1) Test was positive in 99 out 100 patients with MI 2) Test was positive for 12 out 100 in normal controls Test is used in to test 10,000 patients in CCU (35% prevalence) 3500 patients are positive. 3465 are TP PV(+) = TP X 100 TP +FP SENS= TP X 100 TP +FN 99 X 100= 99% 99 +1 PV(+) = 3465 X 100 =81% 3465 +780
Laboratory Test Characteristics Test is then used in to test 10,000 ER patients ( 4% prevalence) 400 patients are positive. 396 are TP PV(+) = TP X 100 TP +FP PV(+) = 396 X 100 =26% 1152 +396 4% prevalence of MI
Efficiency and Receiver Operating Characteristics (ROC) curves Efficiency = TP + TN X 100 TP +FP+FN+TN • Used to differentiate between tests when Sensitivity and Specificity are equally important. • Test with an efficiency of <80 % should not beused ROC curves plots True positive rate to False positive rate for a series of reference values • Useful for assessing the clinical value of different tests • Useful for selecting best Reference value for a test • Recall True positive rate =Sensitivity =TP TP +FN • False Positive rate =FP = 100-specificity FP +TN
ROC Curves Area under the curve .9-1= excellent .8-.9=good .7-.8= fair .6-.7=poor .5-.6=fail sensitivity 1-specificity Shows trade off between specificity and sensitivity Closer the curve follows left-hand border and top border the more accurate the test The closer the test comes to a 45 degree angle the less accurate the test
The Diagnostic Test The view from the laboratory
The Expectation • Clinicians depend on the the laboratory to provide results that are • Accurate • Precise • Timely • Result compared to reference interval and patient is treated accordingly • Result also compared to previous patient results How does the laboratory meet this expectation?
Quality Control (QC) • Quality Control (QC) • The use of statistics, techniques and activities to achieve, sustain and improve the quality of a product or service -Product or Service is the test result The focus of QC in the lab is the method which used to determine the result QC is part of the “Big Picture” of Quality Assurance • Quality Assurance (QA) • Focuses on all aspects of laboratory performance • Analytical results • Overall laboratory Services • Specimen labeling, specimen handling, accurate reporting of test results, TAT, incident reports, patient, nurse or clinician surveys
QC in the Laboratory involves Evaluating method performance Constant Long term Short term So what are we evaluating?
Evaluating method performance • Accuracy • Precision • Sensitivity • Linearity
Evaluating method performance • Accuracy • The closeness of the agreement between the measured value of an analyte and True Value • Gold standard • Comparison to Reference Laboratory • Average of a number of labs
Evaluating method performance • Precision • The ability of an analytical method to produce the same value for replicate measurements of the same sample • With-in run • Between run
Method Sensitivity • The analytical sensitivity of a method refers to the lowest concentration of analyte that can be reliably detected. • The most common definition of sensitivity is the analyte concentration that will result in a signal two or three standard deviations above background. Clinical Sensitivity Vs Analytical Sensitivity
Signal/Noise threshold Signal time
Other measures of sensitivity • Limit of Detection (LOD) is sometimes defined as the concentration producing an S/N > 3. • In drug testing, LOD is customarily defined as the lowest concentration that meets all identification criteria. • Limit of Quantitation (LOQ) is sometimes defined as the concentration producing an S/N >5. • In drug testing, LOQ is customarily defined as the lowest concentration that can be measured within ±20%.
Method Linearity • A linear relationship between concentration and signal is not absolutely necessary, but it is highly desirable. • Ways to evaluate linearity • Visual/linear regression
Signal Concentration
The Application of QC to Laboratory Methods • We base the validity of our patient test result by comparison to other samples analyzed by the same method • Sample Types Analyzed by the Lab • Patient Samples • QC samples • Proficiency samples (PT)
The Application of QC to Laboratory Methods • QC Samples • Samples selected by the laboratory and purchased from an external company • Tested each day of patient testing to mimic patient and proficiency samples • Indicates if the lab’s analytical processes are performing in an acceptable manner, thereby producing clinically acceptable patient and proficiency results • QC samples provide data about accuracy and precision of each methods at the level of analyte present in the control • We interpret the data when making daily decisions about the acceptability of each batch of patient or PT samples
The Application of QC to Laboratory Methods • Proficiency (PT) Samples • External agencies (mandated legislative bodies or voluntary organizations) • QMP LS -Quality Management Program Laboratory Services • Part of Ontario Medical Association (OMA) • CAP College of American Pathologists • Samples are sent to see how well laboratory performs relative to peers and to a defined quality specification. This is usually referred to as a total error allowable (TES) from a target value for each sample. • For many analytes measured a specific license is required • The ability to continue measuring an analyte hinges upon maintaining proficiency
The Application of QC to Laboratory Methods • Running QC and PT samples reflects how well the lab is doing but does not modify or correct or control analytical problems • Require QC system to “drive” the system: • QC data • Rules of acceptability • Tools for monitoring and documenting daily QC and corrective actions
The Application of QC to Laboratory Methods Rules of Acceptability are based upon: • Performance specifications • Numerical limits established by each laboratory for each analyte and each testing system, which often include accuracy, precision, analytical sensitivity (minimum reportable amount), analytical specificity (interfering substances), the reportable range of patient test results and the reference range. • Action Limits • Ranges set for QC samples that if exceeded signal a possible deterioration of the quality of the testing system and requires an investigation by a technologists.
The Application of QC to Laboratory Methods • QC Tools • Levy-Jennings Control Chart • A simple graphical display in which the observed values are plotted versus an acceptable range of values as indicated on the chart by lines for upper and lower control limits • Control Rules • A decision criterion used to interpret QC data and make judgment on the control status • Statistical QC program • Software part of specific analyzer and/or laboratory information system (LIS) which analyzes QC data and provides appropriate feedback • warnings • flags
Levey-Jennings Control Chart +3sd +2sd +1sd mean -1sd -2sd -3sd
Levey-Jennings Control Chart +3sd +2sd +1sd mean -1sd -2sd -3sd
Levey-Jennings Control Chart +3sd +2sd +1sd mean -1sd -2sd -3sd
The Application of QC to Laboratory Methods • Control Rules • Westgard Multirule • A control procedure that uses a series of control rules to test the control measurement. • A 12s rule being used as a warning, followed by the use of 13s, 22s, R4s, 41s and 10x as rejection rules
Westgard Rules 13s refers to a control rule that is commonly used with a Levey-Jennings chart when the control limits are set as measurement exceeds the mean plus 3s or the mean minus 3s control the mean plus 3s and the mean minus 3s. A run is rejected when a single control limit. 12s refers to the control rule that is commonly used with a Levey-Jennings chart when the control limits are set as the mean plus/minus 2s. In the original Westgard multirule QC procedure, this rule is used as a warning rule to trigger careful inspection of the analyte
Westgard Rules 22s - reject when 2 consecutive control measurements exceed the same mean plus 2s or the same mean minus 2s controllimit. R4s - reject when 1 control measurement in a group exceeds the mean plus 2s and another exceeds the mean minus 2s.
Westgard Rules 41s - reject when 4 consecutive control measurements exceed the same mean plus 1s or the same mean minus 1s control limit. 10x - reject when 10 consecutive control measurements fall on one side of the mean.

![Enzyme-Linked Immunosorbent Assay [ ELISA ]](https://cdn1.slideserve.com/2423074/enzyme-linked-immunosorbent-assay-elisa-dt.jpg)