Download
1 / 46
460 likes | 587 Views
Child Welfare Early Intervention Initiative in Philadelphia. Julia Alexander, M.S. Department of Human Services, Philadelphia, PA. Session Outline. Scientific Context: Wellbeing, Risk & Prevention Policy & Law Models & Implementation Responding to Challenges. Children’s Wellbeing.

E N D
Child Welfare Early Intervention Initiative in Philadelphia Julia Alexander, M.S. Department of Human Services, Philadelphia, PA
Session Outline • Scientific Context: Wellbeing, Risk & Prevention • Policy & Law • Models & Implementation • Responding to Challenges
Children’s Wellbeing • Resilience – an individual’s positive adjustment despite experiencing adversity & significant threats to wellbeing • Protective Factors – characteristics located within individuals and their environments that serve to increase resilience and positive adjustment Garmezy, 1970;Masten and Coatsworth, 1998
Resilience • Early examinations of resilience focused on children’s characteristics – e.g., good health, self-regulation, self-esteem, etc. • Subsequent research examined characteristics of families and communities • More recently, resilience is being viewed as multidimensional – children can make positive adaptions in some domains but remain vulnerable in other domains Luthar, Cicchetti & Becker, 2007
Protective Factors • Intelligence – multidimensional! • Temperament – easy, difficult, slow to warm up • Coping styles – talking it out vs. acting out • Positive social support • Racial socialization and racial identity Luthar, Cicchetti & Becker, 2007; Miller, 1999
Scientific Context of Individuals with Disabilities Improvement Act and Keeping Children and Families Safe Act (CAPTA) • Many of the risk factors that are associated with public child welfare system intervention are also associated with developmental delays among infants, toddlers and young children. • Secondary conditions related to early delays include behavioral health problems and poor school achievement. • Strong evidence-base confirming relationships among risk factors and children’s outcomes supported advocates’ efforts to change the law to drive systems’ collaboration. Aber, Jones & Cohen, 2000; Anderson et al, 2003; Bolger & Patterson, 2001.
Eligibility for Part C Infant-Toddler Early Intervention • Presence of a specific developmental delay – cognitive, language, socioemotional, or motor. • Medical condition with a high probability of delay – e.g., Trisomy 21 (Down Syndrome), Failure to Thrive, Fetal Alcohol Syndrome, microencephaly, etc. Judy Silver, Ph.D., The Children’s Hospital of Philadelphia
Risk Factors & Developmental Delay • Other conditions and environmental risk factors associated with delays: • Poverty • Lead exposure • Low birth weight • Parental substance abuse • Exposure to community and family violence
Risk Factors & Developmental Delay • Risk factors are known to: • Occur in clusters • Occur at more than one level of the ecological model (person, family and/or community levels) • Have exponentially cumulative effects Beckwith, 2000; Bronfenbrenner, 1979
Poverty • Infants and toddlers are more vulnerable to the effects of poverty compared to individuals experiencing poverty at later stages of development. • Family characteristics with the strongest relationship to poverty among children under age 5 years are parental education, marital status and employment status.
Poverty • Poverty is also associated with several conditions that raise the risk of poor outcomes • Low birth weight • Lead exposure • Single parent household • Cognitive delays Zeanah, Boris & Larrieu, 1997
Low Birth Weight • Neonatal weight of less than 2500 grams (5 lbs., 8 oz.) affects approximately 10% of live US births. • Advances in neonatal medicine have resulted in increasing numbers surviving. • Increased risk of poor health, sensory impairments, cognitive and motor delays, learning disorders • Cigarette smoking, exposure to alcohol and other drugs, poor maternal health & nutrition and adolescent motherhood are mechanisms linking poverty to low birth weight. Aber, Jones & Cohen, 2000; Meyers, Alexander, Silver & Vogel; Minde, 2000
Lead Exposure • Children most often exposed by eating leaded paint chips or breathing the dust of old deteriorating urban housing. • Urban children have lead levels up to 8 times higher than non-urban children. • Exposure linked to growth stunting, hearing impairments, kidney damage, decreased intelligence scores, reading disorders, behavioral problems, poor achievement. Brookes-Gunn& Duncan, 1997: Lanphear, Dietrich, Auinger & Cox, 2000
Parental Substance Abuse • At least 70% of the families who enter the child welfare system have substance abuse as an issue related to impaired parental role functioning • Families most often headed by single parenting women with a complex array of problems – e.g., abuse, poor educational and employment histories, inadequate housing, etc. • Increased likelihood of child neglect • Women more likely to relapse due to pressures of single parenthood National Center on Addiction and Substance Abuse, 2001; Semidei, Radel & Nolan, 2001
Exposure to Violence - Child Maltreatment • Strongest single predictor of poor outcomes including delays, poor achievement & behavioral disorders • Early discussions focused on the physical injuries of the battered child. • Maltreated children now understood to be at greater risk due to the impact of adverse experiences on their maturing cognitive, emotional and other systems. Kempe et al, 1962; Kim & Cicchetti, 2004
Exposure to Violence – Child Maltreatment • Compromised capacity to resolve stage- salient developmental challenges at their optimal time • Higher likelihood of developmental delays • Higher rates of internalizing and externalizing symptoms, problems with peers, poor school adjustment • Higher likelihood of experiencing other traumatic events – e.g., domestic violence, loss of a parent, etc. Bolger & Patterson, 2001; Kaufman & Henrich, 2000: Rogosch, Cicchetti & Aber, 1995
Cognitive Development & Language Acquisition • Maltreated children less able to using words to describe thoughts and feelings • Study found that maltreated children had smaller vocabularies, less word knowledge and greater rates of syntactic delays • Maltreating mothers’ language impoverished even after controlling for education and socioeconomic status • Sequelae of speech and language problems include learning and behavioral disorders Eigsti & Cicchetti, 2004
Language Development, Maltreatment and School Readiness • School readiness = pre-academic cognitive skills and socioemotional characteristics assess prior to beginning first grade • Emergent literacy = the precursor skills and behaviors that precede formal reading • Emergent literacy facilitated in linguistically rich environments • Knowledge & skills children demonstrate at the start of first grade contributes the most to early academic achievement even when socioeconomic status is controlled Byrnes, 2006; La Paro & Piata, 2000
Language Development, Maltreatment & Self-Regulation • Language acquisition has a strong relationship with socioemotional development • Infants’ cues for care and comfort are among the earliest language precursors. • Caregivers’ interpreting and responding appropriately sets the foundations for more complex preverbal communications. • Insensitive or frightening caregiver responses impact infants’ developing stress regulatory systems. • Fewer resources to devote to typical maturational challenges Prizant, Wetherby & Roberts, 2000
Language Development, Maltreatment & Self-Regulation • Infants’ modulation of arousal is adaptive • Reduces negative affective states • Maintains arousal to an optimal, performance-enhancing range • Supports attention to stimuli • Helps to preserve relationships • Reduces likelihood of behavioral problems Braungart-Rieker & Stifter, 1996; Rothbart & Bates, 1998
Interventions as Protective Factors • Protective factors serve to increase children’s resilience in high risk circumstances and help to avert poor outcomes. • An empirical grasp of protective factors is essential to the task of focusing interventions on areas theory & research suggest will have the most impact Masten & Coatesworth, 1998; Olds, 2005
Interventions as Protective factors • In program planning, nodal points within the ecological/transactional model become the loci of interventions. • Risk factors affecting the caregiving context are transmitted through interactions between parents and their children • Understanding of the role of parents as mediators of risk and children’s outcomes points to the importance of family-focused interventions Sameroff & Fiese, 2000
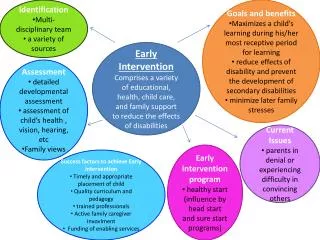
Early Intervention Services • An evidence-based has been established for the efficacy of early intervention services for samples of infants and toddlers who fall within specific disability and risk categories, e.g., cognitive delays, parental substance abuse, etc. Guralnick, 1997
Early Intervention Services • Occupational, Physical, Speech/Language Therapies, Special instruction, Assistive Technology Devices, Nutrition Services • Case management & some health-related services such as transportation assistance • Parent training & support to enhance their child’s development • Respite care. • Spiker & Silver, 1999
Early Intervention Services • In addition to the impact of early intervention on specific areas of delay, services affect mechanisms by which risks are transmitted: • Quality of parent-child interactions (e.g., intrusiveness, sensitivity, etc.) • Parent-mediated play (e.g., developmentally appropriate toys, games, etc.) • Parent-mediated social experiences (e.g., supervised peer interactions, community events, etc.) Guralnick, 1997
Early Intervention Services • Strong philosophical orientation toward caregiver-child relationships and natural environments • Family focus with home visiting improves access and participation • Home setting helps re-distribute the balance of power and support the caregiving role Marcenko, 1999
Objections to Developmental Screening • Concerns about tracking minority children into special education • Historic use of IQ scores to justify racial prejudice (Terman’s revision of Binet scales, 1916) • Mass measurement of intelligence and responses by minority scholars- e.g, George Sanchez, 1932; Horace Mann Bond, 1927; protests of African-American psychology graduate students, 1930’s Guthrie, 1976
What has changed? • Understanding that intelligence is multidimensional – many intelligences rather than a single global factor • The role of environment on development – educational opportunities, cultural values, language, discrimination • Norms developed on more diverse samples
Legislative Support • Adoption & Safe Families Act of 1997 • Keeping Children & Families Safe Act of 2003 • Individuals with Disabilities Act of 2004
Adoption & Safe Families Act of 1997 (ASFA) • Until the passage of ASFA, the objectives of the child welfare system had been child safety and permanency • ASFA included wellbeing as a third objective of child welfare system intervention • Achieving permanency for dependent children in a timely manner became a primary focus of child welfare system to reduce risk of pathology related to disrupted relationships with caregivers Zeanah & Boris, 2000
The Keeping the Children and Families Safe Act of 2003 • Amended the Child Abuse and PreventionTreatment Act (CAPTA) (P.L. 108-36) and requires that each state develop “provisions and procedures for referral of a child under age 3 who is involved in a substantiated case of child abuse or neglect to early intervention services funded under Part C of the Individuals with Disabilities Act (IDEA).”
Individuals with Disabilities Act Part C of 2004 States receiving Part C funds must describe “State policies and procedures that require the referral for Early Intervention services of a child under the age of three who is involved in a substantiated case of abuse or neglect”
Philadelphia Department of Human Services Child Welfare Early Intervention InitiativeModel, Implementation & Preliminary Outcomes
Starting Young Program – Children’s Seashore House of the Children’s Hospital of Philadelphia- Judith Silver, Ph.D., Director • Ages 4 to 33 months • Open Philadelphia DHS cases • Interdisciplinary Pediatric Developmental Evaluations Data and collaboration a major impetus to the Philadelphia Child Welfare-EI Initiative
Systems Change in Philadelphia - 1999 • Integration of the child welfare and behavioral health systems • Establishment of the Behavioral Health & Wellness Center (BHWC) at DHS • Increasing Department of Behavioral Health (DBH) interest in early identification of Pervasive Developmental Disorders/Autism • Increasing opportunities for collaboration and scholarly discourse within DHS/DBH
Infants & Toddlers • Higher vulnerability to the impact of abuse and neglect • Efforts needed to reduce the risks related to cognitive, language and socioemotional delays • Need to determine what interventions may be protective and increase the likelihood of more favorable outcomes In response to these needs and concerns,DHS and DBH proposed the Child Welfare Early Intervention Initiative.
Development of the Model • Informational Brochure (2001) - old unilateral approach • DHS-funded position at ChildLink 2001 in response to anticipated increase in referrals – early partnership of child welfare and early intervention systems • Child welfare system training in EI 2002 – the beginning of full public/private collaboration • Policy Directive 2004 – refer all children 0 – 5 to EI systems for developmental assessments • Policy Directive 2006 – child welfare providers will perform developmental screening and surveillance
Collaborative Partners • DHS – BHWC, Law, Policy • DBH/Mental Retardation Services • ChildLink (0-3 Early Intervention) • Elwyn (3-5 Pre-School Special Education) • PA Council of Children,Youth & Family Services • Private Child Welfare Providers
Program Objectives • DHS Early Intervention ChildFind -Identification of all children 0-5 using administrative database • Developmental screening using the Ages and Stages Questionnaire (ASQ) • Monitoring to ensure that children who need EI and preschool special education continue to receive services • ASQ repeated every 6 months
Policy • Effective December 2004, child welfare providers were directed to assist parents and other caregivers in accessing developmental evaluations for infants, toddlers and young children • Policy revised in November 2006 to require providers to screen (currently undergoing third revision in response to PA State mandate) • Policy requires child welfare providers to monitor the participation of eligible children • Efforts to engage families’ participation needed to be documented in the case record • Collaboration with DHS social work teams when needed to support the participation of children with documented delays and disabilities • Providers given the ASQ and provider directors/managers received training • Providers responsible for training direct service staff
Information Systems • Memo of understanding from DHS permitting ChildLink to use DHS administrative data for Child Welfare Early Intervention Initiative for monitoring purposes • Use of Impromptu (Cognos Corporation, 2004) to generate ChildFind reports for DHS social work teams and child welfare providers • Ability to track referrals by provider • Ability to generatequantitative reports
Provider Training • Overview of the EI and preschool special education systems • Developmental delays, disabilities and the purpose of intervention to promote more developmentally typical outcomes • How to complete referrals and promote participation • ASQ training
New State Policy • Beginning in September 1, 2008, all 67 PA county child welfare systems will be required to use the ASQ to screen infants and toddlers under age 3 years • Addition of the ASQ Social-Emotional Scale • Screening at more frequent intervals
Program Monitoring • DHS is in the process of exploring use of a vender to manage the ASQ data and provide reports to DHS and providers on implementation • Vender will also have the capacity to create aggregate reports
Conclusions • DHS communication with providers • Monitoring one’s own caseload • Call or email with questions or concerns 215-683-5705 or julia.alexander@phila.gov