Download
1 / 26
260 likes | 428 Views
Guidelines for the Use of Antiretroviral Agents in Pediatric HIV Infection Managing Complications of HIV Infection in HIV-Infected Children on Antiretroviral Therapy Pain Management. About This Presentation.

E N D
Guidelines for the Use of Antiretroviral Agents in Pediatric HIV Infection Managing Complications of HIV Infection in HIV-Infected Children on Antiretroviral Therapy Pain Management
About This Presentation These slides were developed using the March 2005 Pediatric Guidelines. The intended audience is clinicians involved in the care of patients with HIV. Users are cautioned that, because of the rapidly changing field of HIV care, this information could become out of date quickly. Finally, it is intended that these slides be used as prepared, without changes in either content or attribution. Users are asked to honor this intent. – AETC NRC http://www.aids-etc.org AETC National Resource Center, www.aidsetc.org
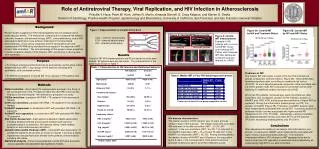
Introduction • Pain is multifactorial, biologically complex • Associated with decreased quality of life, increased mortality, lower CD4% • Common, particularly in younger children and girls • Sources: many, including nerve or muscle inflammation, cardiomyopathy, drug toxicities, invasive secondary infections • Stressors may amplify pain AETC National Resource Center, www.aidsetc.org
Assessment • Self-report • Pediatric visual analogue pain scales and rating systems, modified for age, developmental status, severity of illness, cultural factors • Observational and behavioral assessment • Functional performance • General Health Assessment for Children • Functional Status II (R) AETC National Resource Center, www.aidsetc.org
Principles of Pain Management • Diagnose and treat underlying medical conditions • Involve the child and caretakers in developing strategies • Consider consultation with pediatric pain specialist • Combine nonpharmacologic and pharmacologic therapies AETC National Resource Center, www.aidsetc.org
Nonpharmacologic Interventions • Relaxation techniques, behavior modifications • Environmental management(play, music, scheduled medical/nursing interventions, structured sleep and rest times) • Gentle handling, supportive positioning • Nutritional support, hydration, electrolyte replacement • Optimized tissue perfusion and oxygenation • Transcutaneous electrical stimulation (TENS), massage, whirlpool, physical therapy • Acupuncture AETC National Resource Center, www.aidsetc.org
Pharmacologic Treatment • Dosing guidelines should be consulted, but dosages must be individualized • Effective pediatric analgesic dosage may not be identified(eg, tricyclics, SSRIs, and anticonvulsant medications) • For adjunctive analgesics, analgesic dosage may be lower than the standard dosage for a medication’s primary indication • Start at low dosages, increase as necessary and as tolerated AETC National Resource Center, www.aidsetc.org
Pharmacologic Treatment (2) • Many analgesics undergo hepatic metabolism • May have interactions with PIs or NNRTIs • Analgesic and/or ARV drug levels may be altered • Risk of analgesic toxicity or withdrawal; suboptimal or toxic PI or NNRTIconcentrations AETC National Resource Center, www.aidsetc.org
Types of Medications AETC National Resource Center, www.aidsetc.org
Types of Medications (2) AETC National Resource Center, www.aidsetc.org
Types of Medications (3) AETC National Resource Center, www.aidsetc.org
Special Considerations Opioids • For moderate to severe pain • Excellent analgesia; generally safe • Concurrent use with other agents may enhance analgesia: • GABA agonists, alpha2 agonists, TCAs, SSRIs, anticonvulsants AETC National Resource Center, www.aidsetc.org
Special Considerations (2) Opioid complications: • Excessive sedation • Consider low-dose a.m. stimulants (dextroamphetamine, methylphenidate) • Itching and constipation • Consider very small doses of naloxone • Switch narcotic (eg, to methadone) • Nausea and vomiting • Change narcotic AETC National Resource Center, www.aidsetc.org
Special Considerations (3) Methadone • Has NMDA receptor antagonism • Recommended for long-term treatment of neuropathic pain refractory to nonnarcotics • May induce less tolerance than other narcotics • In adults, may be associated with lower CD4% AETC National Resource Center, www.aidsetc.org
Special Considerations (4) Methadone Switching to methadone from high-dose morphine, Dilaudid, fentanyl • Incomplete cross-tolerance to methadone • Start at LOW dosage(20% of expected equipotent dosage) • Risk of respiratory depression at full equipotent dosage AETC National Resource Center, www.aidsetc.org
Special Considerations (5) Methadone • Some PIs (eg, LPV) and NNRTIs (EFV, NVP) induce metabolism of methadone, lower serum drug levels • Opioid withdrawal symptoms may occur • Higher methadone dosages may be needed • Risk of methadone toxicity if interacting ARVs are discontinued AETC National Resource Center, www.aidsetc.org
Special Considerations (6) Weaning from long-term opioid and benzodiazepine therapy • Minimize physiological stress • Use clonidine (alpha2 agonist), transdermal or oral, to reduce withdrawal symptoms • Transition from IV narcotics to methadone(or fentanyl patch, morphine, MS Contin) • Transition from midazolam to lorazepam AETC National Resource Center, www.aidsetc.org
Special Considerations (7) Weaning from long-term opioid and benzodiazepine therapy • Wean methadone 5-10% every 2-3 days,as tolerated, alternating with 5-10% weanof lorazepam • Wean clonidine at least 3-5 days after discontinuation of narcotics • Assess frequently for withdrawal symptoms AETC National Resource Center, www.aidsetc.org
Special Considerations (8) Escalating narcotic and sedative requirements • Initiate alpha2 agonist and NMDA receptor antagonist • Consider clonidine, dextromethorphan (low-dose) • Substitute methadone for other narcotics, lorazepam for midazolam • Consider rotating narcotics • Consider regional anesthesia for localized pain AETC National Resource Center, www.aidsetc.org
Special Considerations (9) • Analgesia and sedation for painful procedures • For venipuncture: nonpharmacologic interventions plus topical and local anesthesia • For more invasive procedures, consider conscious sedation • Caution with midazolam: levels increased by some PIs and NNRTIs • Caution with fentanyl: respiratory and cardiac depression with loading doses in some patients on PIs or NNRTIs • Start at low dosages, titrate carefully, monitor closely AETC National Resource Center, www.aidsetc.org
Special Considerations (10) • Peripheral neuropathy • Appears to be less severe in children • Lidoderm patch, with other analgesics as needed • Discontinue precipitating medications, if possible • Neuropathic pain • Persists or intensifies independent of ongoing tissue injury or inflammation • May need combination therapy(nonnarcotics with or without narcotics) • Consult pain specialist AETC National Resource Center, www.aidsetc.org
Special Considerations (11) • Movement disorders • Consider levodopa • Consult with neurology, anesthesia, and rehabilitation specialists AETC National Resource Center, www.aidsetc.org
Treatment of Specific Pain Syndromes AETC National Resource Center, www.aidsetc.org
Treatment of Specific Pain Syndromes (2) AETC National Resource Center, www.aidsetc.org
Treatment of Specific Pain Syndromes (3) AETC National Resource Center, www.aidsetc.org
Conclusion • Pain may significantly diminish quality of life and complicate medical management • Optimal management often requires multidisciplinary collaboration(anesthesia, pain service, nursing, social services, others) AETC National Resource Center, www.aidsetc.org