Download
1 / 39
400 likes | 772 Views
Opioid Induced Hyperalgesia. Jill Mosby, MD June 18 th 2008. History OIH. 1880: Rossbach “When dependence on opioids finally becomes an illness of itself, opposite effects like restlessness , sleep disturbance, hyperesthesia, neuralgia, and irritability become manifest” 2. History OIH.

E N D
Opioid Induced Hyperalgesia Jill Mosby, MD June 18th 2008
History OIH • 1880: Rossbach “When dependence on opioids finally becomes an illness of itself, opposite effects like restlessness, sleep disturbance, hyperesthesia, neuralgia, and irritability become manifest” 2
History OIH Six decades later Himmelsbach described opioid abstinence syndrome: “aching in bones, joints, muscles is probably the most common withdrawal symptom” 2
Definitions Analgesia • absence of sense of pain Nociceptive • Causing pain Agonist • a chemical substance capable of activating a receptor to induce a full or partial pharmacological response Antagonist • a drug that counteracts the effects of another drug
More definitions TOLERANCE • Exposure to a drug induces changes that cause decreased response to drug’s effects over time • Can develop quickly or slowly • Cross tolerance can occur (ie: with opioids) SENSITIZATION • A form of nonassociative learning characterized by an increase in responsiveness upon repeated exposure to a stimulus
Standard Risks of Opioid • Physical dependence • Tolerance • Addiction • Overdose • Typical side effects • ? Opioid Induced Hyperalgesia
Opioid Induced Hyperalgesia • Enhanced pain response to a noxious stimulus • Evidence for changes/ source in spinal cord and brain • AKA: Opioid Neurotoxicity
Types of OIH • Maintenance therapy and withdrawal (MW) • Very high dose, or escalating dose (HD) • Ultra-low dose (LD)
Early evidence OIH: MW Rodent Studies Summery • Rodents: mice, rats, guinea pigs • > 75 studies since 1970’s • Multiple opioids (Morphine, Fentanyl, Heroin, experimental) • Multiple routes (IT/SQ/IV/PO/IP) • Time frame of OIH: hours, days, or longer • Pain threshold measured: Mechanical, Electrical or Thermal stimuli This must not be one of the experimental rats…it’s too happy!
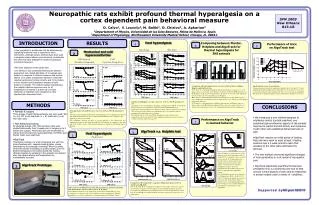
Rat studies: during opioid exposure Vanderah et al, J Neurosc 2001 Angst (chart)
Rats: Persistent hyperalgesia Celerier et al, J Neurosc 2001 Angst (chart)
Rats: Persistent hyperalgesia Celerier et al, J Neurosc 2001 Angst (chart)
Acute hyperalgesia after isolated exposure Celerier et al, Anes 2000 Angst (charts)
Mechanisms studied OIH-MW • Opioid receptors: Mu receptor ↑ • NMDA antagonist (ketamine, MK-801) ↓ • NMDA activation ↑ • PKC inhibition ↓ • IT glutamate/ substance P ↑ • Spinal EAA (increase in chronic opioid use) ↑ • IT Cyclooxygenase inhibitors (NSAID) ↓ • Spinal dynophin ↑ • Spinal cytokines ↑ • IT GM1 ganglioside ? • Dorsal horn Fos-C ? • Hemoxygenase & nitric oxide synthase inhibitors ↓
Evidence for MW in humans • Human studies former opioid addicts • Maintained on methadone vs. no maintenance • Show increased sensitivity to some types of pain
OIH: MW • Surgery pts, volunteer • High vs. low/no opioid dose intraop • Increased postop pain, opioid use in pts received high dose Angst Anesth 2006
Chronic Pain Patients • 6 Pts chronic back pain >6 months • Started on LA morphine • ↓ Tolerance & Threshold of CPP • Pain scores ↓ 30% • Secondary outcomes not changed Angst J Pain 2006
OIH: MW • Human volunteers • Capsaicin-heat for mechanical pain • Pain ↓ remifentanil • Pain & allodynia ↑ after infusion Wood, Anesth Analg
Clinical significance of MW • Argues acute & chronic opioid use may have new risk: OIH (MW) • Opioids may worsen initial pain & ↑ sensitivity to other sources of pain • Query NMDA antagonists future role help prevent OIH
OIH: LD Animal Studies • Animal studies opioid 1000x lower normal dose: OIH to mechanical & thermal • Locally injected LD→hyperalgesia Normal dose→antinociceptic Both reversed with antagonist • Theory: LD opioid trigger excitatory signaling cascade
OIH: LD in Humans • 1940’s study biphasic response to morphine in 7/57 former addicts. Mild hyperalgesia to heat at low dose, analgesia at high dose. • 1979 study showed LD opioid & antagonist had improved post op pain, but was not confirmed repeat studies • No controlled studies in humans
OIH: HD in Animal studies • IT morphine 10x normal: scratching/ biting/ aversion to touch, not resolved with naloxone • IT strychnine: allodynic/ hyperalgesic • Spinal cord EP studies: HD opioids act similar to IT Strychnine • IT injected Glycine: attenuates allodynia
OIH: HD in Animal Studies • 33 opioid related structures studied, characteristic of chemicals produce allodynia/ hyperalgesia: • Phenantrene structure • Hydrogen at position 14 • Ether bond • One or no methyl group on nitrogen • Free 3-OH position ro glucuronide/sulfate conjugate
OIH: HD in humans • Nine case reports pts with allodynia • 22 pts, 8 had myoclonus • Most patients morphine • Routes: PO, IV, IT • Reducing dose opioid or rotation resolved/ reduced sx in 21/22 pts • This is the OIH that is seen clinically in palliative care, ? Rad-Onc
OIH: HD Clinical Picture • Severe allodynia • Intractable, escalating pain on HD/ED opioid • < 50% myoclonus (?), more at rest • Delirium, mental status changes • Increased doses caused ↑ pain • Can lead to sz, coma, death • Reducing dose or rotating opioid reversed sx in almost all patients
Culprit Medications • *Morphine is most common • most used opioid • *Dilaudid • Oxycodone • Less often fentanyl or methadone • * I have seen clinically this year
Mechanism HD • Phenantrene structure linked • NMDA linked, with effects on excitatory signals in CNS • ? Metabolites of opioid (Morphine-3-glucuronide), this is less discussed in literature
Barriers to Treatment • Clinicians often do not know about, recognize, or understand OIH • Family/ patients understanding: How can my Morphine do harm? • Both groups need education
Management of HD • Pain controlled/ mild: ↓ opioid dose • Uncontrolled pain: ↓ dose + adjuvant OR rotate to non-phenantrene opioid • Benzodiazapines • Fluids • Educate Davis M, Walsh D
Bottom Line • Future of pain control will be greatly influenced by this area of research • Peripheral nerves, spinal cord & CNS all involved in OIH • Chronic pain could be worsened by acute and ongoing opioid therapy
Bottom Line (cont’d) • For Patients with resistant/ escalating pain, hyperalgesia should be considered • OIH (HD) treat with decreased opioid dose or rotation to another opioid • I hope this has given some insight into some of the challenges in treating pain • I hope this helps you recognize OIH (HD)
Questions to ponder • Opioid tolerance & hyperalgesia linked? • Worsening chronic non-malignant pain? • Are there genetic differences that cause OIH MW & HD? • What is on horizon to help HD OIH? Ketamine like medication?
Bibliography • Angst MA, Clark JD: Opioid induced hyperalgesia. Anesth 2006; 104: 570-87 • Mercandante S, Ferrera P, et al: Hyperalgesia: an emerging Iatrogenic Syndrome. J Pain and Sympt Management 2003; 2: 769-775 • Davis MP, Shaiova LA, Angst MS: When opioids cause pain. 2007; 25: 4497-4498 • Chang G, Chen L, Mao J: Opioid tolerance and hyperalgesia. 2007; 91: 199-211
Bibliography • Ballantyne JC, et all: Opioid Induced Hyperalgesia. Pain: Clinical Updates 2008; 16: 1-4 • Celerier E, Rivat C, et al: Long-lasting Hyperalgesia Induced by Fentanyl in Rats. Anesth 2001; 92: 465-72 • Celerier E, Laulin JP, et al: Progressive Enhancement of Delayed Hyperalgesia Induced by Repeated Heroin Administration: a Sensitization Process. J Neurosc 2001; 21: 4074-80 • Chu LF, Clark DJ, et al: Opioid Tolerance and Hyperalgesia in Chronic Pain Patients after one month of oral morphine therapy: a preliminary prospective study. J Pain 2006; 7:43-48 • Hood DD, Curry R, Eisenach JC: Intravenous remifentanyl produces withdrawal hyperalgesia in volunteers with capsaicin-induced hyperalgesia. Anesth Analg 2003; 97: 810-5