Download
1 / 18
180 likes | 206 Views
Is Propofol Safe and Effective for Procedural Sedation in the Emergency Department?. February 21, 2007. Propofol (Diprovan). Short acting non-opiod sedative hyptonic Potentiates γ -amino butyric acid in CNS Onset: <60 seconds Duration: ~5-10 minutes

E N D
Is Propofol Safe and Effective for Procedural Sedation in the Emergency Department? February 21, 2007
Propofol (Diprovan) • Short acting non-opiod sedative hyptonic • Potentiates γ-amino butyric acid in CNS • Onset: <60 seconds • Duration: ~5-10 minutes • Procedural sedation dose: 1 mg/kg IV bolus • Gastroeneterologists, dentists, radiologists
ProSCED Registry Acad Emerg Med. 2007 Jan;14(1):41-45.
Propofol For Emergency Department Procedural Sedation--Not Yet Ready For Prime Time. • Cautionary editorial • Risk of oversedation • Personnel requirements • Fasting in setting deep sedation • Recommended large case series Acad Emerg Med. 1999 Oct;6(10):975-978.
Propofol in Emergency Medicine: Pushing the Sedation Frontier Ann Emerg Med. 2003 Dec;42(6):792-797.
Propofol in Emergency Medicine: Pushing the Sedation Frontier • Review of literature through 2003: 11 studies involving about 1000 patients • “…we now have enough evidence for propofol to be an acceptable standard of care (like ketamine and fentanyl/midazolam) in emergency medicine.” Ann Emerg Med. 2003 Dec;42(6):792-797.
Propofol for Emergency Department Procedural Sedation and Analgesia: A Tale of Three Centers • Prospective descriptive consecutive series • 3 centers, 792 patients, ages 0.5-90 years • Propofol 1mg/kg, then 0.5mg/kg prn, mean dose 1.8mg/kg • Orthopedics, cardioversion, incision and drainage Acad Emerg Med. 2006 Jan;13(1):24-30
Propofol for Emergency Department Procedural Sedation and Analgesia: A Tale of Three Centers • No intubations, no prolonged obs, no admissions • “All propofol related procedural sedation events resolved with brief supportive interventions in the ED with no adverse sequelae.” Acad Emerg Med. 2006 Jan;13(1):24-30
Propofol Versus Midazolam/Fentanyl for Reduction of Anterior Shoulder Reduction • Multicenter randomized blinded clinical trial • 2 centers in Australia • Adults with anterior shoulder dislocation • Propofol (n=48) • Midazolam/Fentanyl (n=38) Acad Emerg Med. 2005 Jan;12(1):13-9.
Propofol Versus Midazolam/Fentanyl for Reduction of Anterior Shoulder Reduction • Propofol: quicker full wakefulness (p<0.001) • Propofol: easier reduction (p=0.047) Acad Emerg Med. 2005 Jan;12(1):13-9.
Propofol Versus Midazolam/Fentanyl for Reduction of Anterior Shoulder Reduction • Not powered to examine secondary outcomes • Propofol: less reduction attempts (p=0.02) Acad Emerg Med. 2005 Jan;12(1):13-9.
Propofol Versus Midazolam/Fentanyl for Reduction of Anterior Shoulder Reduction “Propofol appears to be as effective as midazolam/fentanyl for reduction of anterior shoulder dislocation…however, the advantage of shorter wakening times should be weighed against the possibility of adverse events, particularly respiratory depression and vomiting” Acad Emerg Med. 2005 Jan;12(1):13-9.
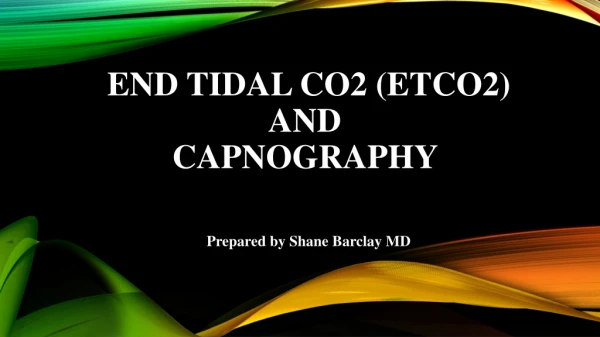
Randomized Clinical Trial of Etomidate Vs Propofol For Procedural Sedation in the ED • Randomized non-blinded prospective trial • Hennepin County Medical Center • Adult patients only • Propofol (n=109) 1 mg/kg + 0.5 mg/kg • Etomidate (n=105) 0.1 mg/kg + 0.05 mg/kg Ann Emerg Med. 2007 Jan;49(1):15-22.
Randomized Clinical Trial of Etomidate Vs Propofol For Procedural Sedation in the ED Ann Emerg Med. 2007 Jan;49(1):15-22.
Randomized Clinical Trial of Etomidate Vs Propofol For Procedural Sedation in the ED Ann Emerg Med. 2007 Jan;49(1):15-22.
Randomized Clinical Trial of Etomidate Vs Propofol For Procedural Sedation in the ED “Etomidate and propofol appear equally safe for ED procedural sedation; however, etomidate had a lower rate of procedural success and induced myoclonus in 20% of patients” Ann Emerg Med. 2007 Jan;49(1):15-22.
HUPism Propofol is safe and effective for procedural sedation when used by Emergency Physicians. We should actively work to get access to propofol in the HUP ED.
Propofol Syndrome • Arrythmia during propofol infusion plus 1 or more of the following: • Lipemic plasma • Hepatomegaly or hepatic steatosis • Metabolic acidosis • Rhabdomyolysis with myoglobinuria • Inhibition of mitochondrial free fatty acid metabolism • Long term continuous infusions, > 5mg/kg/hr, critically ill patients on steroids and/or pressors