Download
1 / 14
140 likes | 284 Views
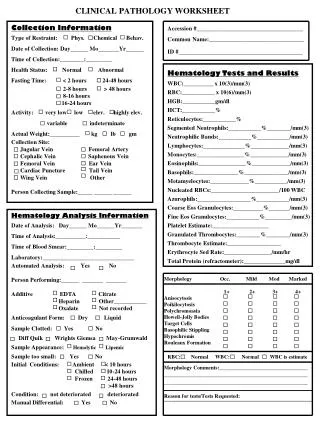
D.H. Clinical Pathology Conference August 21, 2015. Stella Lai MD Ronald Hamilton MD. HPI.

E N D
D.H.Clinical Pathology ConferenceAugust 21, 2015 Stella Lai MD Ronald Hamilton MD
HPI 29 yo M w/ h/o ulcerative colitis, basal cell carcinoma and metastatic melanoma who presented to ED for diffuse HA, nausea, transient visual disturbance (flashing lights in L upper visual field), transient L hand numbness + tingling, speech difficulty and acute onset confusion.
Other History PMHx/PSHx HTN Nephrolithiasis Ulcerative Colitis Basal Cell Carcinoma s/p resection Metastatic Melanoma w/ known brain, lung, chest wall, lymph node, thigh and gluteus involvement s/p numerous biopsies + resections and treatment w/ IL2, aflibercept, dendritic cell vaccine +/- interferon booster and pembrolizumab
Allergies Ativan (parodoxical agitation) Meds Vitamin B6, Vitamin B12, Vitamin D, Vitamin E, MV, Dexamethasone Taper, Keppra 1000mg BID, Mesalamine 4800mg QHS, Zofran PRN, oxycodone PRN Social Hx Lives w/ wife. No smoking, alcohol or illicits. Family Hx Mother: Prothrombin Gene Variant w/ h/o DVT/PE Maternal GM: Breast Cancer @ 55
Exam VS: 37.2, BP 143/90, HR 98, RR 17, O2 Sat 97% RA MS: Alert and oriented x 3, Agitated, Repetitive/slow/labored speech, Follows simple commands CN: VFs intact, PERRL, EOMI, No facial asymmetry MOTOR: 5/5 strength throughout SENSORY: Intact to light touch throughout REFLEXES: 2+ biceps/triceps/patella/achilles, No ankle clonus, No Hoffmans COORDINATION: ? GAIT: ?
Clinical Localization ….of confusion, diffuse headache, nausea, speech difficulty (sounded like it was mostly expressive), L hand numbness/tingling and L upper VF flashing lights.
Hospital Course Received 10mg IV Decadron and 25g IV mannitol in ED, and was admitted for further management. He was continued on Decadron 4mg IV 6 hours and returned back to baseline 24 hours after admission. He was d/ced on dexamethasone slow taper w/ instructions for repeat brain MRI in 1 month.
Hospital Course 2 months later, he presents w/ acute abdominal pain. It was initially tolerable but progressed to stabbing, 10/10 pain that was not responsive to oxycodone. CT abdomen revealed L renal vein thrombosis and diffuse metastatic disease. He was initially placed on heparin gtt which was stopped b/c of his known hemorrhagic metastatic brain lesions. He underwent repeat neuroimaging.
Hospital Course 3 days after admission, abdominal pain acutely worsened. CT abdomen revealed free air and small bowl perforation. Not a surgical candidate b/c of hemodynamic status. The next day, he arrested (?2/2 PE) requiring 30 minutes of CPR for ROSC. He was intubated and maxed out on 3 pressors. Given poor prognosis, he was made CMO and expired.
Pathology Gross Pathology Well-demarcated lesions Variable amount of pigmentation Could be hemorrhagic and necrotic Micro Pathology Pleomorphic Melanocytes Mitosis Necrosis Staining + for S-100, HMB-45, Melan-A
Virtual Microscopy • 2D H&E • 2D MITF • 2D Tyrosinase • 2I H&E • 2I LFB/PAS • 2J H&E