Download
1 / 92
1.74k likes | 5.82k Views
FURCATION INVOLVEMENT AND ITS MANAGEMENT. CONTENTS. Introduction Definition Clinical features Microscopic features Terminology Anatomy Classification Anatomic considerations Etiology of furcation invasions Diagnosis. Treatment Scaling and rootplaning Obliteration of furcation

E N D
CONTENTS Introduction Definition Clinical features Microscopic features Terminology Anatomy Classification Anatomic considerations Etiology of furcation invasions Diagnosis
Treatment Scaling and rootplaning Obliteration of furcation Gingivectomy/apically positioned flap Furcationplasty Tunnel proceedure Resective periodontal proceedures Regenerative proceedures Tooth extraction Prognostic factors Conclusion
Molars are the tooth type demonstrating the highest rate of periodontal destruction in untreated disease and suffer the highest frequency of loss for periodontal reasons Furcation involvement is defined as bone resorption and attachment loss in the interradicular space that results from plaque-associated periodontal disease. Such a condition is reported to considerably increase the risk for tooth loss. Therefore, furcation defects represent a formidable problem in the treatment of periodontal disease, principally related to the complex and irregular anatomy of furcations..
Moreover, the responsiveness to therapy may be complicated by the presence of a greater radicular surface potentially offered to bacterial toxins and calculus buildup ,as compared to defects surrounding single-rooted teeth. Once the lesion has established, the discrepancy in extent between the root surfaces and the periodontal soft tissues facing the bacterial insult may be responsible for a reduced healing response. Finally, the distal location in the arch and the difficult access may conceivably impair both self-performed and professional plaque control procedures in the furcation area, limiting their effectiveness
Definition : • The term Furcation involvement refers to the invasion of the bifurcation and trifurcation of multi-rooted teeth by periodontal disease. • The mandibular first molars - most common sites and maxillary premolars - least common • Increases with age.
Clinical Features • Microscopic Features
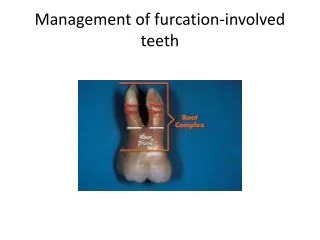
Terminology : • Root complex is the portion of a tooth that is located apical of the cementoenamel junction (CEJ) i.e., the portion that normally is covered with a root cementum Root trunk Root cone
The furcation is the area located between individual root cones • Furcation is divided into 3 parts Roof -which is the base of the root trunk and contains bifurcation ridge. Flute -usually concave or grooving of the root trunk, extending from the cervical line and blending into the actual furca. Inter-radicular area or the area of the root separation or furcation chamber,
Degree of separation : the angle of separation between two roots (cones). • Divergence : is the distance between two roots • Coefficient of separation : the length of the root cones in relation to the length of the root complex.
Glickman (1958) Staffileno (1969) Goldman and Cohen's (1980) • Heins & Canter (1968) • Hamp et al (1975) • Lindhe & Nyman (1975) • Ramjford & Ash (1979) • Riccheti (1982) • Lindhe (1983) • Tarnow & Fletcher (1984) • Hou et al (1998)
Glickman (1958) • Grade-I: When there is soft-tissue lesion or pocket extending into the flute of the furcation, but the inter-radicular bone is intact. This involvement of the periodontium in the furcation area is without manifested radiographic evidence of bone loss. • Grade-II: Loss of inter-radicular bone & pocket formation of varying depths into the furcation but not completely through the opposite side of the tooth. • Grade-III: Complete loss of inter-radicular bone with radiographic evidence presenting a small triangular radiolucency at the furcation area. There is a pocket formation that is completely probable to the opposite side of the tooth. However, the furcation is not visible clinically. • Grade-lV: Same features as those of Grade III except that loss of periodontal attachment & gingival recession has made the furcation clearly visible to a clinical examination.
Hamp et al (1975) • Degree I / class 1: represents horizontal attachment loss of less than 3 mm within the furcation involvement. • Class-II: represents horizontal loss greater than 3 mm but not encompassing the total width of the furcation. • Class-III: denotes horizontal through and through destruction. This classification is similar to that described by Lindhe & Nyman (1975).
Tarnow & Fletcher (1984) – millimeters. • Subclass A: Vertical destruction to one third of the total inter radicular height (1 to 3 mm). • Subclass B: Vertical destruction reaching two thirds of the inter radicular height (4 to 6 mm). • Subclass C: Inter radicular osseous destruction into or beyond the apical third (> 7 mm).
Anatomic considerations: • 1) Root trunk length and Entrance width • 2) Concavity of the inner surface of exposed roots • 3) Degree of separation of the roots • 4) Bifurcational ridges • 5) Enamel projections • 6)Accessory pulp canals
1) Root trunk length and Entrance width: short root trunk – furcation become involved early in the disease process. long root trunk – furcation -invaded later - more difficult to reach and instrument. First molars generally have shorter root trunks than second molars.
) Concavity of the inner surface of exposed roots: exhibit - an occluso-apical direction. This may make instrumentation for calculus removal and root planing almost impossible. First molars frequently have plaque harboring concavities, especially the mesiobuccal roots of maxillary molars and the mesial roots of mandibular molars. This may allow bacterial plaque, its toxins and ultimately calculus to penetrate for into the root surface making the removal difficult.
3) Degree of separation of the roots: Wide separation of the roots improves access, thereby facilitating instrumentation. First molar furcations are frequently wider than those of second molars. • 4) Bifurcational ridges: Buccal and lingual ridges were found in 63% of the mandibular molars. These ridges resulted in the roof of the furcation being located more coronally than the entrances.
5) Enamel projections: AAP - enamel pearl is "a small focal mass of enamel formed apical to the CEJ", while enamel projection is "an extension of the cervical enamel margin either toward or into the root furcation area ". Master & Hoskins (1964) grade I, short CEP from CEJ grade II, longer CEP and approaches the furcation area grade III, CEP that extends directly into the furcation. These occur in approximately 15% of molars. They favour plaque accumulation and must be removed to facilitate scaling and root planing.
6) Accessory pulp canals: The presence of accessory pulpal canals in the furcation area may extend pulpal inflammation to the furcation. 28% to 59% of the molar have been found to have accessory pulp canals.
Etiology of furcation invasions • Primary factor - Bacterial plaque • Predisposing factors - Anatomical considerations Root concavities Enamel pearls and projections Accessory pulp canals Bifurcation ridges Location of furcation relative to CEJ Location and diameter of furcation entrance Extension of inflammatory periodontal disease
Isolated molar furcation invasions Trauma from occlusion Pulpal periodontal disease Iatrogenic cofactors Root fractures involving furcations
Trauma from occlusion: Predisposing co factor - more rapid formation of furcation involvement is controversial. The molar furcation is unique compared with a single rooted tooth in that its periodontal ligament between the crest of the interfurcal bone & the dome of the furcation is aligned in a horizontal rather than a vertical plane. Thus, even slight increase in centric occlusal forces would have the same crushing effect on periodontal ligament as destructive, lateral forces on a PDL aligned in a vertical plane. .
Because molar teeth are closer to the condyle the forces generated on them are much higher than those on more anterior teeth. Therefore trauma from occlusion combined with deeper inflammation in close proximity to a furcation results in rapid loss of attachment than from inflammation alone. The greater susceptibility of molar teeth to traumatic forces could be a reason for the formation of an isolated furcation involvement
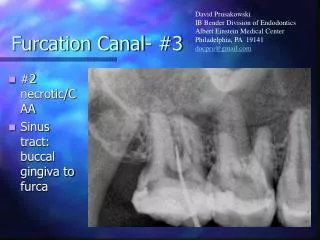
Pulpal periodontal disease: The high percentage of molar teeth with patent accessory canal opening into the furcation suggests that pulpal disease could be an initiating cofactor in the development of furcation involvement. Accessory canals connecting the pulp chamber floor to the furcation have been found in 36% maxillary first molars, 12% of maxillary second molars, 32% of mandibular first molars and 24% of mandibular second molars.
latrogenic cofactors: Overhanging restorations harbor - dental plaque - periodontal inflammation and attachment loss. A study of molars with and without crowns and proximal restorations found that molars with restorations had a higher prevalence of furcation involvement and greater attachment loss
Root fractures involving furcations: Rapid, localized, alveolar bone loss is often seen associated with vertical root fractures. If these root fractures involve the trunk of a multi-rooted molar and extend into a furcation, a rapidly forming isolated furcation defect can result. The prognosis for these situations is poor and usually results in loss of the tooth.
Clinical diagnosis • Radiographic diagnosis
CLINICAL DIAGNOSIS: • Cardinal symptoms: Redness and swelling increased temperature pain and lossof function In advanced cases, the closed topography of the roots of a multirooted tooth may even promote the development of a painful periodontal abscess.
Clinical probing: The buccal furcation entrance of the maxillary molars and the buccal and lingual furcation entrances of the mandibular molars are normally accessible for examination using a curved graduated periodontal probe, an explorer or a small curette. In maxillary molars - mesial furcation should be probed from the palatal aspect of the tooth. The distal furcation entrance of the maxillary molar - probed from either the buccal or the palatal aspect of the tooth.
Straight periodontal probes are used clinically to determine the height and width of furcation involvement - less useful for determining the degree of horizontal involvement. Tibbetts (1969) recommended the use of a curette to negotiate the curve of furca and Carranza (1979) advocated the use of a curved Cowhorn explorer or Nabers probe. Carranza stated that furcas can best be evaluated with a curved Nabers probe.
The probing of vertical attachment loss on the roots adjacent to furcation involvement is also important. Vertical attachment loss on the adjacent roots should be probed at the furcation line angle of each root, angling the probe somewhat into the furca. To determine the bone contours associated with furcation involvement more accurately, transgingival probing or bone sounding can be accomplished through anesthetized soft tissues.
ATTACHMENT LOSS: A more specific feature of the furcation lesion is the development of horizontal attachment loss which means that the pocket has a lateral extension. The molar furcations present a complex anatomical configuration that makes recording pocket depths and attachment levels more difficult. Also the clinical probing is generally hampered by the soft tissues bordering the areas to be probed. Clinical attachment levels are usually measured with a straight_probe. It is obvious that a straight probe would not be able to reach the full extent of furcation defect because the initial vertical pocket curves horizontally into the furca.
for this purpose a curved Nabers probe or a fine curete is very useful. The curvature of these instruments allows them to be passed under the roof of the furca and to measure the horizontal and vertical degree of involvement. Carranza stated that furcas can best be evaluated with a curved Nabers #2 probe. Also there are calibrated furcation probe ZA - 2 with calibrations in 2 mm increments, ZA - 3 with calibrations in 3 -mm increments.
The clinical examination of furcas on the approximal tooth surfaces may be more difficult when neighboring teeth are present, especially if the contact area between the teeth is large. This is particularly the case in maxillary molars. The clinical examination of maxillary premolars is often difficult due to limited access for probing. It may not always be possible - until flap is raised in an explorative (surgical) procedure in the area.
Radiographs: Furcation involvements are often first detected on radiographs if they have been made before probing measurements are obtained. Maxillary furcations are not readily seen in radiographs taken at right angles to the teeth and suggested that better visualization of the furcations is possible by varying the angle of the beam. They recommend using a film holder to allow the use of long cone, right angle techniques. Lateral and vertical x-ray beam deviation can grossly distort the furcation image leading to false interpretations. Glickman found that clinically significant tissue changes in the furcation often are not detected by radiographs.
On x-ray films of maxillary molars, a small, triangular, radiolucent shadow is sometimes seen over the mesial or distal roots in the proximal furcation areas, which has been called furcation arrow. The association of this image with deep grade II or grade III Furcation involvement was significant compared with uninvolved furcations, but the arrow was not seen in more than half of the sites with a deep grade II furcation involvement and in slightly less than half of grade III sites. Thus, it appears that radiographs alone do not detect furcation involvement with any predictable accuracy and that probing the furcation area is necessary to confirm the presence & severity of furcation involvement.
Three diagnostic criteria suggested to assist in radiographic detection of furcation involvement: 1) The slight radiographic change in the furcation area should be investigated clinically, especially if there is bone loss on adjacent roots. 2) Diminished radiodensity in the furcation area in which outlines of bony trabeculae are visible suggests furcation involvement. 3) Whenever there is marked bone loss in relation to a single molar root, it may be assumed that the furcation is also involved.
MANAGEMENT OF FURCATION • Can be broadly classified as put forth by Kalkwarf and Reinhardt (1988) as follows. • Maintain the furcation • Increase the access to furcation • Removal of furcation • Closure of furcation with new attachment.
Three broad strategies of furcation therapy are: I. Maintenance of the existing Furcation: Scaling and root planing Obstruction of the Furcation II. Increasing access to the Furcation: Gingivectomy/Apical positioned flap Odontoplasty . Osteoplasty/Ostectomy III. Elimination of the Furcation Root amputation/ Tooth resection Bicuspidization
Degree 1 • SRP (scaling & root planing) • Flap curettage • Apically positioned flap • Odontoplasty • Osteoplasty, Ostectomy • Degree II • Flap curettage • Root resection • Hemisection • Flap curettage with barrier membrane (GTR) • Degree III • Flap curettage • Root resection • Hemisection • Flap curettage with barrier membrane (GTR) • Strategic extraction
SCALING AND ROOT PLANING : It can be closed or open. I) Non- surgical/Closed scaling and Root Planing: Indicated for Grade I and shallow Grade II furcations. Closed scaling and root planing may be the treatment of choice if surgery is contraindicated for medical or psychological reasons.
II) Surgical/Open Scaling and Root planing: If sufficient subgingival access with a closed approach is not possible, for furcated molars with deep lesions, then open scaling using flap procedure such as modified widman flap yields more effective calculus removal
OBLITERATION OF THE FURCATION - OCCLUSIVE BARRIER filling of advanced furcation defects with biocompatible material to eliminate anatomic niches in which bacteria accumulate.. Potential advantages of an occlusive barrier: • Easy to place into furcation • Doesn’t require a suture for stability. • Elimination of a second stage procedure
Doesn’t require complete coverage by the gingival flap • Bacteriostatic. • Lower cost. • No chance of transmission of viral infection