Download
1 / 22
250 likes | 633 Views
Cervical Nerve Root Impingement By: Michael Cox. Overview . Anatomy of cervical spine and nerve roots Reasons for impingement Signs and symptoms associated with nerve root impingement Acute treatment of injury Rehabilitation Return to play criteria. Anatomy .

E N D
Overview Anatomy of cervical spine and nerve roots Reasons for impingement Signs and symptoms associated with nerve root impingement Acute treatment of injury Rehabilitation Return to play criteria
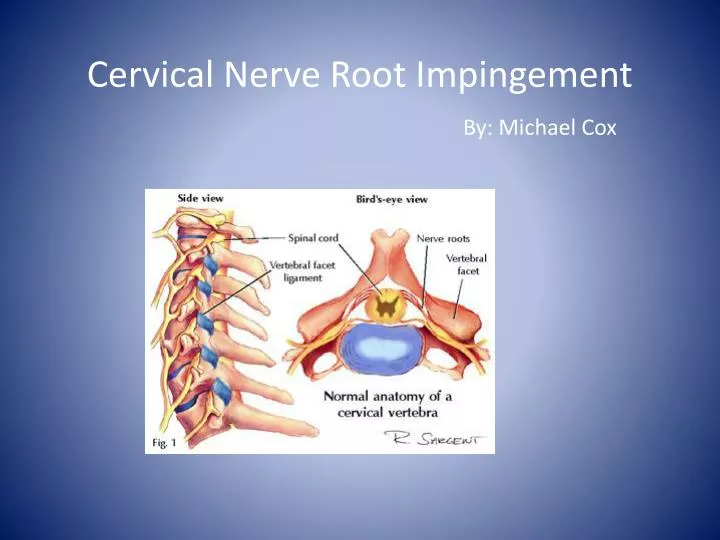
Anatomy • Primary Function: Mobility, support, and protection of spinal canal and neural structures • 7 cervical vertebrae • 8 nerve roots • 6 intervertebral discs • Foramina • Nerve root occupies 25-33% over the foramina space • Lordotic curve • most of lordosis occurs at C1-C2 • Some Biomechanics: • 50% of flexion and extension occurs at occipitoatlantal joint • 50% of rotation occurs at C1-C2
Anatomy • Vertebral Disc • Located between C2-C7 • Composed of annulus fibrosis, which is the outer layer made up of thick fibrous cartilage • Nucleus pulposus is the inner layer which is a water gelatin • Discs serve as shock absorbers and allow the spine to bend
Anatomy • Nerve roots • Myotomes • C1: Cervical flexion • C2: Cervical flexion • C3: Cervical lateral bending • C4: Shoulder elevation • C5: Shoulder Abduction • C6: Elbow Flexion/wrist extension • C7:Elbow extension/wrist flexion • C8: Ulnar deviation/thumb extension • T1: Finger abduction/adduction • Dermatomes • C1: Top of head • C2: Side of face • C3: Down mandible • C4: Lateral neck • C5: lateral upper arm • C6: Lateral forearm to thumb • C7: Middle forearm to 3rd • C8: 5th to medial forearm • T1: Medial upper arm
Anatomy • Muscles • SCM • Splenius muscles • Levator scapula • Scalenes • Upper trapezius
Mechanism for Impingement • This injury can occur from an extension, lateral bending, or rotation mechanism, which causes a narrowing of the neural foramen and results in ipsilateral nerve root injury • Disc herniation can cause the nucleus pulposus to leak into the foramen and cause impingement on the nerve
Signs and Symptoms • Neck and shoulder pain and discomfort that can radiate down the arm • Tingling or numbness along the nerve root involved • Motor weakness in affected nerve root (manual muscle testing) • Depending on reason for impingement certain motions (AROM) can cause pain • Point tenderness is usually located along the lateral and posterior cervical muscles on the affected side • Muscle tenderness and spasm on affected side is usually present
Special Test’s • Deep Tendon Reflexes • Biceps Brachii reflex: C5-C6 • Brachioradialis reflex- C5-C6 • Triceps reflex: C7-C8 • Foraminal Compression Test • Manuel Distraction • Shoulder Abduction Test
Acute Treatment • “A best-evidence synthesis by the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and its Associated Disorders concluded that there is not clear evidence that surgical treatment of cervical radiculopathy provides better long-term outcomes than nonoperative measures.” • Icing • NSAIDS • Rest • Take measures that reduce force compressing the nerve root • Avoiding positions that increase symptoms
Rehabilitation Early Phase • Main goal is reducing symptoms: controlling pain and inflammation • Cervical collar • Restricts motions that cause pain • Patient comfort • Cervical pillow at night can help can help maintain the neck in a neutral position and limit head positions that cause narrowing of the neural foramen • Ice- help reduce muscle spasm and pain • NSAIDS
Rehabilitation Early Phase • Traction- Decreases pressure caused by axial loading • Manuel traction • Mechanical traction • Positional traction • Self administered, body positioning Disc Protrusion- Intermittent traction • Force pulposus back in Impingement- Sustained traction • Removes mechanical pressure on nerve root and allows for inflammation of nerve root to decrease • Reducing adhesions within Dural sleeve by elongating the surrounding structure • Restoring normal slack in the neuromeningeal structures
Rehabilitation Moderate Phase • Goals: • Restoring ROM • Maintaining pain free symptoms • Light strengthening • Criteria for progression • Pain and inflammation have been controlled
Rehabilitation Moderate Phase • Continued Traction • Stretching: • Sustained stretching in all directions • Flexion, extension, lateral bending, rotation • Home stretching exercises • Soft Tissue Mobilizations • Spleni muscles, posterior cervical muscles, scalenes, upper trap, levator scapulae, SCM • AROM exercises • Go until pain then return to neutral • All directions
Rehabilitation Moderate Phase • Joint Mobilizations • Cervical lateral glides in upper limb neurodynamics position • Upper and Midthoracic spine manipulation in supine: • “an association exists between mobility in the thoracic spine and neck/shoulder pain.” • “thoracic manipulation can help increase cervical ROM” • Central PA’s
Rehabilitation Moderate Phase • Strengthening • At this time rehab should focus on isometric strengthening only until full ROM is achieved • Flexion • Extension • Lateral bending • Rotation • Deep flexor strengthening • Scapular muscle strengthening • Rhomboids: rows • Serratus anterior: push up plus • Middle and upper trap: fly’s
Rehabilitation Progressive Phase • Goals: • Maintain ROM • Maintain pain free symptoms • Cervical muscle strengthening • Cervical Stabilization • Nerve root strengthening • Functional Activity • Criteria for progression • Pain free ROM • Diminished inflammation
Rehabilitation Progressive Phase • Strengthening: • Isotonic cervical strengthening • All directions: can be done using a cervical machine, pulley system, or Thera-band • Involved nerve root strengthening • Isotonic motions • Can use either dumbbells, Thera-band, tubing, mechanically
Rehabilitation Progressive Phase • Cervical stabilization • All directions • Hold for 30 sec • 3 sets • PNF Patterns • Functional Activity
Return to Play Criteria • Full pain-free ROM • Full strength and stabilization • No tingling or numbness with ROM • Full cardiovascular endurance
Summary • Cervical nerve root impingement can occur from a herniated disc or from narrowing of the neural foramen • Patient may complain of neck pain and tingling or numbness radiating down the arm • Progression is based on patient symptoms • Pain management is important