Download
1 / 36
360 likes | 505 Views
Hypermobility syndrome. Its impact on the young patient. Pam Baxter MSc CPD evening 14 th January 2013. Edinburgh Branch SOCAP. Welcome!. Format of presentation: Ok Podiatrists have a good understanding of this phenomenon. But lets revisit!

E N D
Hypermobility syndrome.Its impact on the young patient. Pam Baxter MSc CPD evening 14th January 2013. Edinburgh Branch SOCAP.
Welcome! • Format of presentation: • Ok Podiatrists have a good understanding of this phenomenon. But lets revisit! • Tonight I want to focus on the Child’s experience. • Why? Because they are often overlooked and therefore help comes late!
Style • CPD event. • Reflective practice • Anecdotal • Case history • Later we take a look at symptoms, briefly management and where to locate more information.
Content. • Information is multisource. • MSc and focus groups • Patients • Journals, text books. • Web sites and media.
Hypermobility syndrome. • For many children joint hypermobility does not cause problems. • However this condition can result in a very miserable child. Significantly affecting their daily life. • If a young patient complains about sore legs, please don't assume they're just being lazy.
The following is a description of a patient who is struggling to get a diagnosis. • This is a classic case!!!!! • A nine-year-old girl, complained that the sole of her left foot was sore, and a large lump had formed in the medial arch. • Visiting the GP- these symptoms were put down to the ill-fitting shoes (she lived in Ugg boots all the time)!
The GP’s advice…. • GP said the footwear was unsupportive, and the boots had appeared to have irritated the arch of her foot, that is why it was inflamed. • The advice was: Get rid of the boots and it will all settle. • The Uggs were duly binned, and parents and patient waited for the swelling to go down.
However…..no change! • Instead, the lump got bigger until it became so painful the girl couldn't walk. • A trip to casualty resulted in crutches, but no answers. • The girl was examined by several doctors and the foot was X-rayed. • Nobody could work out what this lump was. • And the parents were urged to get a referral to an orthopaedic surgeon.
Several weeks later…. • The girl was still in constant pain. • No diagnosis. • No resolution of symptoms. • Mum “Her passion was dancing, so to see her on crutches was heartbreaking”.
What happened at orthopaedics? • Mum talking about the consultant- “Well, he wiggled her feet around, bent her knees and manipulated her arms before taking hold of one of her hands”.
And… • Mum continues “Watch this,” he said, and promptly bent her thumb so far back that it touched her wrist. • “ I was horrified”…….. • “I then realised my daughter hadn't so much as flinched. Nor did she when he bent her whole hand back until it was almost flat”.
A diagnosis then? • “She's double-jointed” the consultant said. • “Your daughter has hypermobility syndrome,” he explained. • “In other words, she's super bendy”.
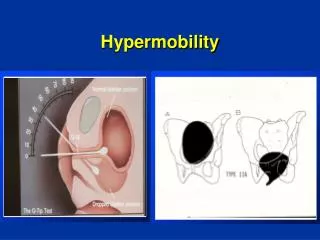
Hypermobility syndrome. • Hypermobility syndrome (HMS)? • Many HCPs describe the patient as double-jointed. • Why are they double jointed? The collagen in the ligaments in their joints is far more flexible than it should be. • Hypermobility goes beyond the normal flexibility enjoyed by the young. • The joints have double or more the range of movement than they should.
What advice was given? • Mum queries.. • “Well, being hypermobile had weakened my daughters ankles, making her turn in on her feet as she walked. And a recent growth spurt made this worse” ?
What caused the pain then? • Mum “Well, eventually a scan showed she had a stress fracture in a long bone in her foot.” • Mum “I was told lots of people are double-jointed and to varying degrees; but hypermobility syndrome can create all sorts of problems”.
MSc research? • I will come back to mum and daughter later. • Qualitative research…..focus groups. Looking at different health care professionals (HCP) attitude to patients with overly flexible joints. • Generally poor! Podiatrists one the best!
Specialists in the field are growing in number. • Prof Rodney Grahame is still one of those consistent voices talking about HMS. • A consultant rheumatologist at University College Hospital, London and the Hypermobility Clinic at Great Ormond Street • Although, he still believes the medical community still hasn't got to grips with hypermobility.
Mis-information • For example… • Prof Grahame: “Many doctors reassure patients that HMS disappears before adulthood.” That’s not the case. • It may decrease in intensity, but adults with HMS still suffer with pain and are at increased risk of dislocations, stress fractures, frozen shoulder and carpal tunnel syndrome.
The HMS patient. • This person is prone to all manner of soft-tissue injuries. • Such as severe bruising around the joints. • Which is why children, and adults should avoid showing off their bendy joints!
Children with HMS • Unfortunately kids who complain are often dismissed, ignored, or just fail to get noticed. • In the UK approx. 15 -30 per cent of children have the condition, which can affect just one or two joints or every joint in their body. • Clinical scoring systems - 4 joints or more, pain for 3 months plus.
Symptoms (child) • Stamina can be affected. • Enthusiasm can be diminished about joining in ... “I don’t do p.e.” “Things are just sore all over, tired……….” “My feet wobble” “ I can’t keep up” • Muscle weakness so prone to injury. • Muscle pain (muscle spasm) • Movement pain. (Writing …..sport) • Joint pain very common. • Many children suffer from dislocations. • Soft-tissue injuries. Stress fractures.
Growing pains then? • The symptoms are often put down to growing pains or simply having a moany child. • Prof Grahame – “A child's muscles aren't strong enough to cope with the fact that their connective tissues are so flexible. They have to work incredibly hard just to put one foot in front of the other and stay upright”.
And so…. • He says that by the evening the child is often exhausted. • It's like when someone first goes to the gym - they may lie in bed aching after that activity. • A child with HMS will feel like that most nights.
Back to our…. Mum • “As a toddler my daughter would cry for her pushchair after walking the shortest of distances. When she got older she would sob during family walks, saying her legs hurt. My husband and I put it down to laziness and told her she was being a wimp.” • “She complained of sore arms and legs at bedtime, she said it was stopping her from getting to sleep, I thought she was playing up and told her to stop making a fuss.”
Clumsy? • Mum “My daughter is also very clumsy - she's forever knocking things over”. • Professor Grahame states that children with HMS are clumsy because their sense of where things are around them is impaired. • Co-ordination is poor and they appear gangly. This is because they don't have enough control over their limbs and often fall as a result.
I asked earlier what should a podiatrist be aware of? • What’s normal for a child? • I am often asked, how do you know if your young patient is hypermobile? And not just very flexible because of their young age? • Get a detailed patient history! Get the clues. • Explore the day to day experiences. What appears normal for your young patient……
pGALS • Paediatric • Gait • Arms • Legs • Spine • Tells you what is normal
Clinical Scoring? • Beightons vs Brighton Criteria vs Bulbena Criteria???????? • For ease stick with Beightons.
Some facts to remember. • The average age of when children start to complain is about 6 years. • But the age at diagnosis is most likely to be 9 years—(a 2- to 3-year delay in diagnosis). • Major presenting complaints: • History of joint dislocation. • Arthralgia (74%). ( More than one joint). • Abnormal gait. • Apparent joint deformity (10%). • Back pain (6%). • Information from Medscape Dr Adib (Manchester Uni).
Also. • Rheumatologists consider that HMS is usually hereditary and can appear as a symptom of other serious conditions, such as Ehlers-Danlos syndrome, Osteogenesis Imperfecta, and Marfan syndrome. • Here an early diagnosis and treatment are advised. • So ask parents when taking that history!
Management 1 Prevention of injury! • HMS is normally managed through exercise and physiotherapy, to treat physical problems involving the body’s systems such as the musculoskeletal, cardio vascular and respiratory. • Core stability-pilates.
Management 2 • Medication • PRICE • Surgery ? • Many HCP involved: OTs • Podiatrists - attempt to normalise gait, making it more efficient, less energy being expended. Orthoses usually very successful.
Patient education. • ARC no longer exists. • Arthritis Research UK has taken its place. • HMSA “Hypermobility Syndrome Association”. • Has a section dedicated to the younger patient /teenager.
CPD on HMS • Short course for health practitioners. • Where: University of Hertfordshire • What: “Hypermobility Symposium” • When: March 2013
Thanks for listening.The end. Thanks!