Download
1 / 34
350 likes | 705 Views
Motion Capture Analysis of Subthalamic Nucleus Deep Brain Stimulation in Parkinson's Disease. Dunbar Alcindor MD Allegheny General Hospital 12/8/2012. Disclosures. None. Parkinson’s Disease (PD) .

E N D
Motion Capture Analysis of Subthalamic Nucleus Deep Brain Stimulation in Parkinson's Disease Dunbar Alcindor MD Allegheny General Hospital 12/8/2012
Disclosures • None
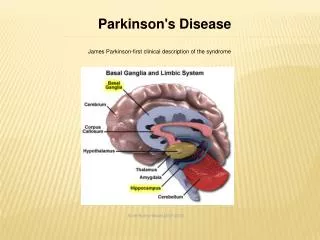
Parkinson’s Disease (PD) • PD is a progressive neurodegenerative disorder associated with a loss of dopaminergic neurons in substantia nigra par compacta. • It affects approximately 1% of individuals older than 60 years. • Cardinal features include resting tremor, rigidity, bradykinesia, and postural instability.
Parkinson’s Disease-Treatment • The goal of medical management is to provide control of signs and symptoms for as long as possible while minimizing adverse effects. • Medications usually provide good symptomatic control of motor signs for 4-6 years.
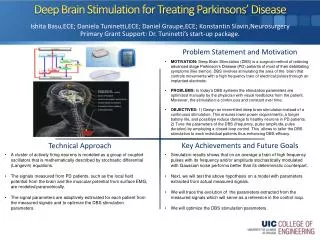
Parkinson’s Disease-Treatment-Deep Brain Stimulation (DBS) • The subthalamic nucleus (STN) most common site for DBS-PD • STN-DBS has been shown to improve motor activity and ADL • The Unified Parkinson’s Disease Rating Scale (UPDRS), most common and well established measurement tool.
The Unified Parkinson’s Disease Rating Scale (UPDRS) Total UPDRS consists of four parts • Parts I, II, and III contains 44 questions each measured on a 5-point scale (0-4). • I. Mentation, behavior, and mood • II. Activities of daily living (ADL) • III. Motor function • IV. Complications of therapy
UPDRS Part III • 14 sections • Score 0-52
The Unified Parkinson’s Disease Rating Scale (UPDRS ) • UPDRS scale has several limitations: • Inherent subjectivity • Requires specialized training to administer the test. • Early and mild motor disability with PD may not be detected with the UPDRS
Motion Capture • Motion capture in movies, military , sports and medicine • Avatar • Star wars • Pirates of the Caribbean
Objective • Can motion capture provide objective measures of a subject’s response to DBS treatment for Parkinson’s disease?
Methods • 6 Subjects (3M,3F) • Idiopathic PD dx 8-16 yrs(mean 11 yrs) • Age range 51-67 years (mean 58 yrs) • Post DBS-STN 2-5yrs (mean 3.3 yrs) • Single surgeon and center • Dr. D.M. Whiting, Allegheny General Hospital
Methods-MC • Kinematic data from 6 subjects (3M/3F) were recorded using a motion capture system consisting of 16 Vicon Vx infrared cameras. • The cameras record the 3-dimensional location of 60 reflective markers placed on the participant's body at 120 Hz.
Methods-MC • Participants walked along a walkway(3 meters) at a self selected pace. • Medications withheld 12 hours prior to study • Pts were assessed with stimulator on and then off • 30 minutes between testing • Study approved by AGH and CMU IRB
Methods • UPDRS Part III Motor component • Tremor- hands and feet • Action tremor • Hand pronation/supination • Gait • Arise from chair • Postural stability • Leg agility
Methods • UPDRS Part III Motor component • Tremor- hands and feet • Action tremor • Hand pronation/supination • Gait • Arise from chair • Postural stability • Leg agility
Methods • UPDRS Part III Motor component • Tremor- hands and feet • Action tremor • Hand pronation/supination • Gait • Arise from chair • Postural stability • Leg agility
Methods • UPDRS Part III Motor component • Tremor- hands and feet • Action tremor • Hand pronation/supination • Gait • Arise from chair • Postural stability • Leg agility
Methods • UPDRS Part III Motor component • Tremor- hands and feet • Action tremor • Hand pronation/supination • Gait • Arise from chair • Postural stability • Leg agility
Methods • UPDRS Part III Motor component • Tremor- hands and feet • Action tremor • Hand pronation/supination • Gait • Arise from chair • Postural stability • Leg agility
Methods • UPDRS Part III Motor component • Tremor- hands and feet • Action tremor • Hand pronation/supination • Gait • Arise from chair • Postural stability • Leg agility
Results-UPDRS • UPDRS Scores for 6 subjects • Stimulator on and off • Average score On 1.5 and Off 15.3
Results-Gait Analysis • DBS-STN On • Stride Length • Walked Faster • Tasked completed in less time Blue = Off Green = On
Results-Gait Analysis • When stepping patterns were assessed, subjects took longer steps
Results- Gait Analysis • Walked faster and completed their assigned task in less time in the On state
Results-Gait • MC stepping patters during 3 meter walk
Correlation of UPDRS Part III Motor Scores with DBS in On and Off Condition • On-Positive Correlation: • Step Height Variance • Speed Variance • Off -Positive Correlation: • Step width
R Wrist acceleration during walking • Less oscillations, more fluid movement -On LWrist acceleration during walking
Pelvis Accelerations • The pelvis angle(rad) recorded during walking in the Off state was lower and distance between peaks wider for AP and vertical accelerations. • Similar for both in M-L accelerations.
Heel Clearance • Improved heel clearance seen with stimulator On • This was seen irrespective of R/L • Patients were able to raise their feet higher • Took less time to raise their feet
Conclusion • UPDRS correlated when DBS-On for step height and speed, and DBS – Off for step width • MC in DBS-STN subjects in On State • Improved heel clearance • Wrist: Less oscillations, more fluid movements • Pelvis: more control and consistency • In AP and vertical acceleration during assigned walking task • Patients took less steps, longer strides and completed task in less time
Conclusion • MC may be utilized to provide a non-invasive and quantifiable method of motor assessment in PD. • Our preliminary evidence suggest that MC may be more sensitive to certain motor problems than the UPDRS • MC data may someday be used to improve DBS parameter programming.
Future Studies-MC and PD • How can we more accurately capture the cardinal symptoms of PD • Disease Progression • Overall effect of treatment • Are there any other subtle signs and symptoms that we can capture to accurately predict disease course
Acknowledgements • Allegheny General Hospital-Division of Neuromodulation • Dr. D.M. Whiting • Dr. M.Y. Oh • Dr. N.D. Tomycz • Dr. B. C. Cheng • Allegheny General Hospital-Dept of Neurology-Movement Disorders Section • Dr. S. Baser • Carnegie Mellon University- Robotics and Computer Science Department • Dr. J. Hodgins • L. Trutoiu