Download
1 / 1
10 likes | 150 Views
ONCOLOGICAL REFERRAL PATTERNS OF GYNAECOLOGICAL CANCER PATIENTS OVER 2010 – 2011 THE NEED FOR GYNAECOLOGIC ONCOLOGY SUBSPECIALITY SERVICES Asma Tanvir Usmani, Samra Ayub, Ayesha Basharat Benazir Bhutto Hospital, Rawalpindi, Pakistan. OPTIONAL LOGO HERE. OPTIONAL LOGO HERE. INTRODUCTION.

E N D
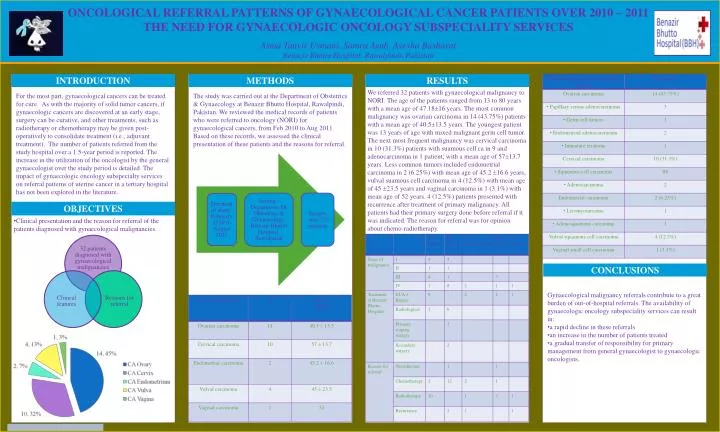
ONCOLOGICAL REFERRAL PATTERNS OF GYNAECOLOGICAL CANCER PATIENTS OVER 2010 – 2011THE NEED FOR GYNAECOLOGIC ONCOLOGY SUBSPECIALITY SERVICES Asma Tanvir Usmani, Samra Ayub, Ayesha BasharatBenazir Bhutto Hospital, Rawalpindi, Pakistan OPTIONALLOGO HERE OPTIONALLOGO HERE INTRODUCTION METHODS RESULTS For the most part, gynaecological cancers can be treated for cure. As with the majority of solid tumor cancers, if gynaecologic cancers are discovered at an early stage, surgery can be curative, and other treatments, such as radiotherapy or chemotherapy may be given post-operatively to consolidate treatment (i.e., adjuvant treatment). The number of patients referred from the study hospital over a 1.5-year period is reported. The increase in the utilization of the oncologist by the general gynaecologist over the study period is detailed. The impact of gynaecologic oncology subspecialty services on referral patterns of uterine cancer in a tertiary hospital has not been explored in the literature. The study was carried out at the Department of Obstetrics & Gynaecology at Benazir Bhutto Hospital, Rawalpindi, Pakistan. We reviewed the medical records of patients who were referred to oncology (NORI) for gynaecological cancers, from Feb 2010 to Aug 2011. Based on these records, we assessed the clinical presentation of these patients and the reasons for referral. We referred 32 patients with gynaecological malignancy to NORI. The age of the patients ranged from 13 to 80 years with a mean age of 47.1816 years. The most common malignancy was ovarian carcinoma in 14 (43.75%) patients with a mean age of 40.513.5 years. The youngest patient was 13 years of age with mixed malignant germ cell tumor. The next most frequent malignancy was cervical carcinoma in 10 (31.3%) patients with suamous cell ca in 9 and adenocarcinoma in 1 patient; with a mean age of 5713.7 years. Less common tumors included endometrial carcinoma in 2 (6.25%) with mean age of 45.2 16.6 years, vulval suamous cell carcinoma in 4 (12.5%) with mean age of 45 23.5 years and vaginal carcinoma in 1 (3.1%) with mean age of 52 years. 4 (12.5%) patients presented with recurrence after treatment of primary malignancy. All patients had their primary surgery done before referral if it was indicated. The reason for referral was for opinion about chemo-radiotherapy. OBJECTIVES • Clinical presentation and the reason for referral of the patients diagnosed with gynaecological malignancies. CONCLUSIONS • Gynaecological malignancy referrals contribute to a great burden of out-of-hospital referrals. The availability of gynaecologic oncology subspeciality services can result in: • a rapid decline in these referrals • an increase in the number of patients treated • a gradual transfer of responsibility for primary management from general gynaecologist to gynaecologic oncologists.






