Download
1 / 23
230 likes | 436 Views
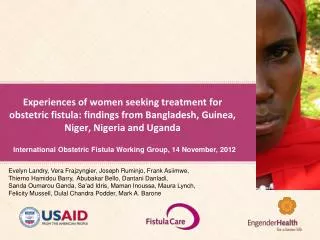
immediate management of the obstetric fistula. kees waaldijk MD PhD babbar ruga fistula teaching hospital. the management of the obstetric fistula starts the moment the leaking of urine is manifest. prevention of the fistula is a utopia for at least another century

E N D
immediate management of the obstetric fistula kees waaldijk MD PhD babbar ruga fistula teaching hospital
the management of the obstetric fistula starts the moment the leaking of urine is manifest • prevention of the fistula is a utopia for at least another century • prevention of the woman from becoming an outcast is very well feasible by the immediate management by: catheter and/or early closure • waiting 3 months is malpractice since one allows the woman to become an outcast by pure neglect of the fistula
the management of the obstetric fistula starts the moment the leaking of urine is manifest if no fistula expertise available: • do not waste valuable time • insert FOLEY catheter Ch 18 for 4 weeks • high oral fluid intake of 6-8 liters per day • ensure free urine drainage preferably free into pot • no routine antibiotics since it is pressure necrosis • antibiotics only on indication, e.g. puerperal sepsis • immediate mobilization of patient, if necessary with stick • oral iron preparations; systemic if needed • high protein diet
the management of the obstetric fistula starts the moment the leaking of urine is manifest if surgical expertise available • vaginal examination for assessment • insert FOLEY catheter Ch 18 • examine patient_fistula once a week • if it seems healing leave catheter in situ • if not healing excise slough and prepare for early closure • as soon as wound clean perform an early closure • mobilize patient at all times • attend to the other needs of the patient
mass campaign immediate indwelling bladder catheter at least 25-30% will be cured with a minimum of 25,000 a year
immediate managementcatheter and/or early closure4,424 patientskano/katsina1984 thru 2008 • total of 13,800 procedures • in total of 11,460 patients • 4,424 immediate management • 39% of patients and 32% of procedures
immediate indwelling catheter2,031 patients • total procedures: 13,800 • total patients: 11,460 • immediate management: 4,424 • immediate catheter: 2,031 • 18% of patients and 15% of procedures • 46% of immediate management
resultsin 2,031 catheter treatments • total no of patients: 2,031 • completely healed/dry: 1,579 (78%) • kano: 705 (82%) healed/dry out of 864 patients • katsina: 875 (75%) healed/dry out of 1,167 patients
catheter treatment as start of immediate management • total immediate management: 4,424 • immediate catheter: 2,031 (46%) • cured by catheter: 1,579 (36%)
catheter treatmentin relation to total number of patients • total no of procedures 13,800 • in total no of patients 11,460 • catheter treatment 2,031 • 18% of patients • 15% of procedures
catheter resultsin relation to total number of patients • total no of procedures 13,800 • in total no of patients 11,460 • healed/dry by catheter 1,579 • 14% of patients • 11.5% of procedures
mass campaignimmediate indwelling bladder catheter • implement that any woman gets an indwelling bladder catheter the moment leakage of urine starts; with an annual incidence rate of 80,000 to 100,000 • then at least 25-30% would be prevented from developing a fistula: minimum of 25,000/year • which is more than all operations by all fistula surgeons in the world combined
indwelling bladder catheter andhigh oral fluid intakeat 15 days and at 43 days
necrotic lesions vulva, sphincter ani rupture with atonic bladderat 11 days debridement
catheter, sitzbath with detergent9 days later at 20 days repeat debridement
16 days later at 27 dayspatient sent home at 2 mth with healed wounds
everything healedat 4 mth; and 16 days after sphincter ani repairreported back at 10 mth with amenorrhea of 3 mth
failed catheter treatmentat 21 days; 8 days after debridement